

Concurrent IgA Nephropathy and Membranous Nephropathy, Is It an Overlap Syndrome?
- PMID: 35359934
- PMCID: PMC8961684
- DOI: 10.3389/fimmu.2022.846323
Concurrent IgA Nephropathy and Membranous Nephropathy, Is It an Overlap Syndrome?
Erratum in
-
Corrigendum: Concurrent IgA nephropathy and membranous nephropathy, is it an overlap syndrome?Front Immunol. 2023 Jun 9;14:1218427. doi: 10.3389/fimmu.2023.1218427. eCollection 2023. Front Immunol. 2023. PMID: 37359520 Free PMC article.
Abstract
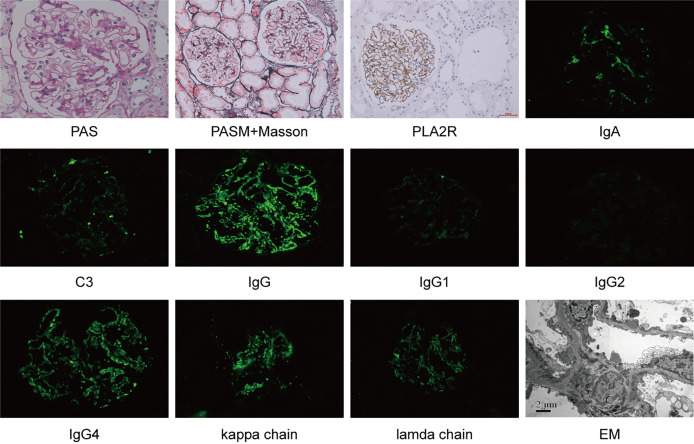
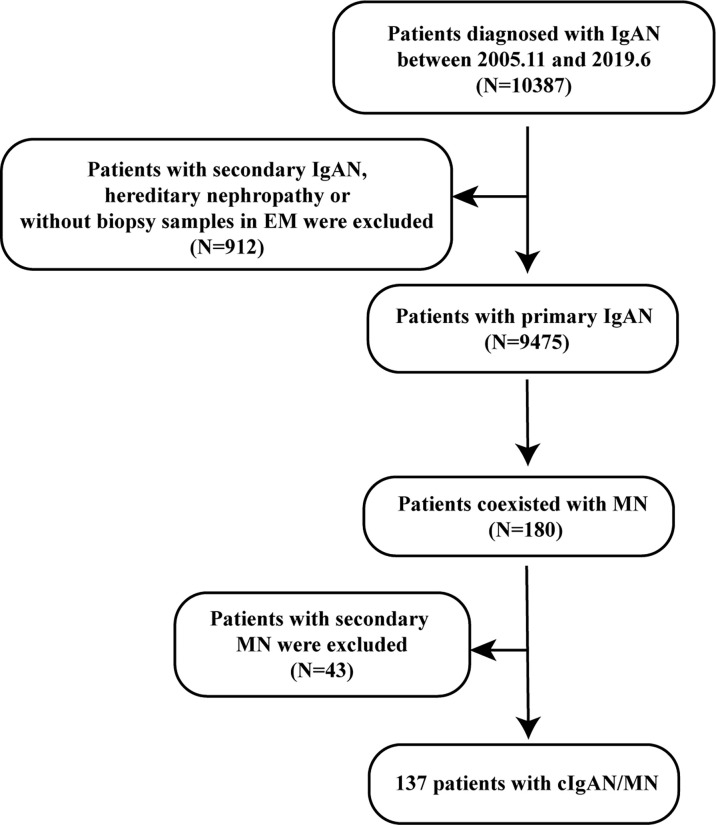
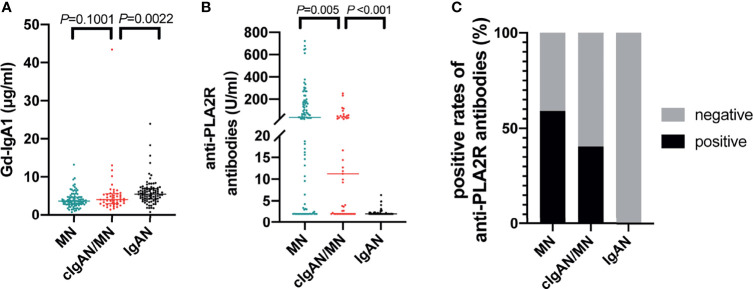
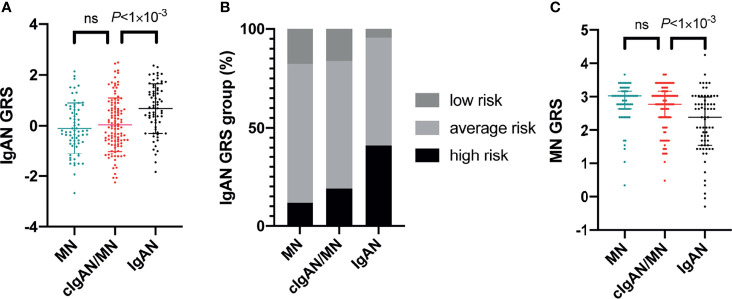
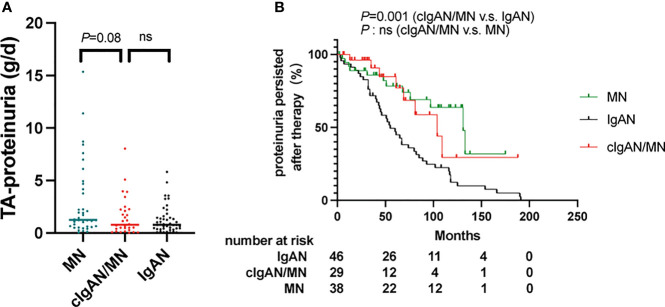
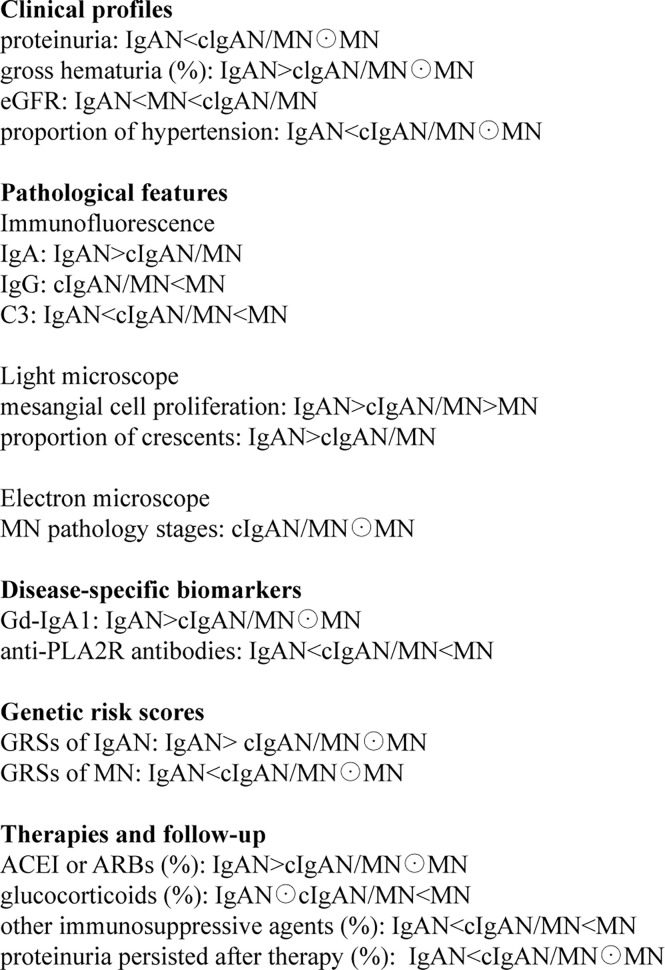
IgA nephropathy (IgAN) and membranous nephropathy (MN) are common glomerulonephritis, the presence of which in the same patient- concurrent of IgAN and MN (cIgAN/MN) has been described occasionally. This study aims to show clinical-pathological features of cIgAN/MN and attempts to suggest underlying pathogenesis using disease-specific biomarkers and a genomics approach. This retrospective cohort study described the clinical and pathological data from 137 patients with cIgAN/MN diagnosed in Peking University First Hospital from 2005 to 2019. One hundred primary IgAN and 100 MN cases were randomly selected as disease controls between the same time interval. Moreover, disease-specific biomarkers and polygenic risk score models were conducted to reveal the underlying pathogenesis. The median age of the cIgAN/MN cases was 45-year-old, and 46% were women. Compared to IgAN, patients with cIgAN/MN had a higher level of 24-hour proteinuria excretion but lower microscopic hematuria. They had a lower median level of galactose-deficient IgA1 (Gd-IgA1, 4.00 versus 5.45 μg/ml, P=0.002) as well as the standardized genetic risk scores of developing IgAN (GRSs: 0.05 versus 0.68, P<0.001). Compared to MN, patients with cIgAN/MN had a lower proportion of nephrotic syndrome and a lower level of albumin-to-creatinine ratio. However, the 24-hour proteinuria levels, serum lipid profiles, proportion of hypertension, and pathology classification were similar. Patients with cIgAN/MN had lower levels of plasma autoantibodies against the M-type transmembrane phospholipase A2 receptor (PLA2R) (11.23 versus 36.59 U/ml, P=0.005). Intriguingly, there were no statistical differences in standardized GRSs of developing MN between them (2.77 versus 3.02, P=0.326). Compared to IgAN, cIgAN/MN may lean towards MN more according to clinical-pathological features, disease-specific biomarker levels, and disease-specific genetic risk scores.
Keywords: IgA nephropathy; anti-phospholipase A2 receptor; galactose-deficient IgA1; polygenic risk score; primary membranous nephropathy.
Copyright © 2022 He, Cui, Zhou, Chen, Li, Zhang, Wang, Gan, Liu, Shi, Zhu, Hou, Lv and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Comment in
-
IgA nephropathy associated with anti-PLA2R antibody positive: a case report.Int Urol Nephrol. 2022 Nov;54(11):3043-3044. doi: 10.1007/s11255-022-03242-0. Epub 2022 May 19. Int Urol Nephrol. 2022. PMID: 35588342 No abstract available.
References
-
- Floege J, Barbour SJ, Cattran DC, Hogan JJ, Nachman PH, Tang SCW, et al. Management and Treatment of Glomerular Diseases (Part 1): Conclusions From a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int (2019) 95:268–80. doi: 10.1016/j.kint.2018.10.018 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous