

B-Lymphocytes in the Pathophysiology of Pancreatic Adenocarcinoma
- PMID: 35359944
- PMCID: PMC8963963
- DOI: 10.3389/fimmu.2022.867902
B-Lymphocytes in the Pathophysiology of Pancreatic Adenocarcinoma
Abstract
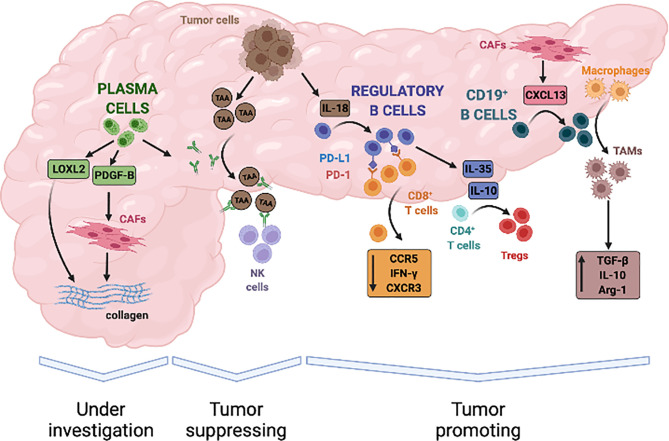
Pancreatic adenocarcinoma is highly infiltrated by B lymphocytes but the relevance of these immune cells in tumor development has been surprisingly overlooked until recently. Based on available evidence from other solid tumors, interaction between B lymphocytes and neoplastic cells is probably not uniformly stimulatory or inhibitory. Although presentation of tumor antigens to T cells and production of antitumor immunoglobulins might intuitively suggest a prominent tumor suppressive activity, specific subsets of B lymphocytes can secrete growth factors for neoplastic cells and immunosuppressive cytokines thus promoting escape from immunosurveillance and cancer progression. Because many of these mechanisms might also be implicated in the development of PDAC, and immune-modulation of B-cell activity is nowadays possible at different levels, determining the role of B-lymphocytes in this lethal cancer becomes of utmost importance to design novel therapeutic strategies. This review aims to discuss the emerging role of B cells in PDAC tumorigenesis, progression, and associated stromal reaction.
Keywords: B cells; B lymphocyte; PDAC - pancreatic ductal adenocarcinoma; cancer associated fibroblast (CAF); fibrosis; pancreatic adenocarcinoma.
Copyright © 2022 Minici, Testoni and Della-Torre.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Hruban RH, Takaori K, Klimstra DS, Adsay NV, Albores-Saavedra J, Biankin AV, et al. . An Illustrated Consensus on the Classification of Pancreatic Intraepithelial Neoplasia and Intraductal Papillary Mucinous Neoplasms. Am J Surg Pathol (2004) 28:977–87. doi: 10.1097/01.pas.0000126675.59108.80 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical