

Transradial versus Transfemoral Access and the Risk of Acute Kidney Injury following Primary Percutaneous Coronary Intervention in Patients with ST-Elevation Myocardial Infarction: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Propensity-Score-Matched Studies
- PMID: 35360090
- PMCID: PMC8930211
- DOI: 10.1155/2022/6774439
Transradial versus Transfemoral Access and the Risk of Acute Kidney Injury following Primary Percutaneous Coronary Intervention in Patients with ST-Elevation Myocardial Infarction: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Propensity-Score-Matched Studies
Abstract
Objectives: The aim of this study is to examine the association between vascular access sites and the incidence of AKI in patients with STEMI undergoing primary PCI.
Background: Emerging evidence has suggested that transradial access (TRA) may be associated with lower rates of acute kidney injury (AKI) as compared with transfemoral access (TFA). However, most of these studies have included a nonselected study population undergoing diagnostic cardiac catheterization or percutaneous coronary intervention (PCI). Data on the association between TRA and AKI in this setting of STEMI are limited and with conflicting results.
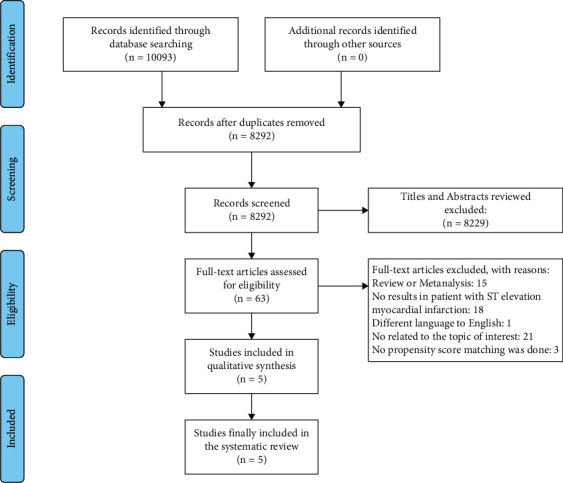
Methods: We systematically searched PubMed, Embase, and Scopus for abstracts and full-text articles from inception to July 13th of 2021. Studies included were randomized controlled trials (RCTs) and propensity-score-matched (PSM) studies evaluating the association of TRA versus TFA access with AKI in patients undergoing primary PCI for STEMI. Data were integrated using the random effects model and generic inverse-variance method of DerSimonian and Laird.
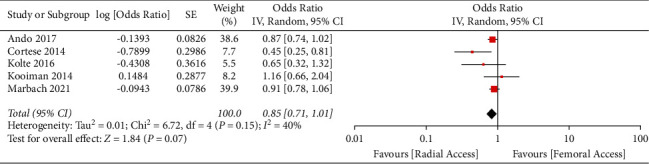
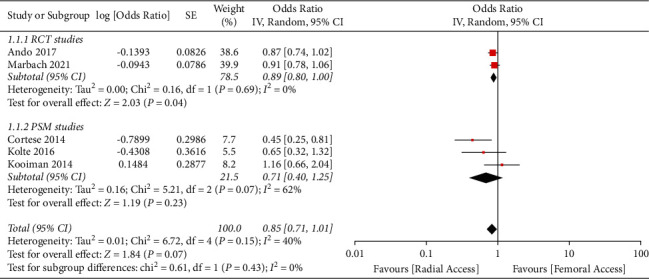
Results: A total of 10,093 studies were found. After applying our inclusion criteria, 5 studies from 2014 to 2021 with a total of 8,536 STEMI patients were included. TRA was not significantly associated with a reduced risk for AKI compared with TFA (odds ratio 0.85, 95% CI 0.71-1.01, p 0.07, I 2 = 40%).
Conclusions: Transradial access was not significantly associated with lower risk of AKI in patients undergoing primary PCI for STEMI compared with TFA. Larger studies are needed to clarify this outcome.
Copyright © 2022 Gaspar Del Rio-Pertuz et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Association of radial versus femoral access with contrast-induced acute kidney injury in patients undergoing primary percutaneous coronary intervention for ST-elevation myocardial infarction.Cardiovasc Revasc Med. 2016 Dec;17(8):546-551. doi: 10.1016/j.carrev.2016.07.008. Epub 2016 Jul 21. Cardiovasc Revasc Med. 2016. PMID: 27566903
-
Impact of Access Site Practice on Clinical Outcomes in Patients Undergoing Percutaneous Coronary Intervention Following Thrombolysis for ST-Segment Elevation Myocardial Infarction in the United Kingdom: An Insight From the British Cardiovascular Intervention Society Dataset.JACC Cardiovasc Interv. 2017 Nov 27;10(22):2258-2265. doi: 10.1016/j.jcin.2017.07.049. JACC Cardiovasc Interv. 2017. PMID: 29169494
-
Impact of vascular access on acute kidney injury after percutaneous coronary intervention.Cardiovasc Revasc Med. 2016 Jul-Aug;17(5):333-8. doi: 10.1016/j.carrev.2016.03.004. Epub 2016 Mar 10. Cardiovasc Revasc Med. 2016. PMID: 27050627
-
Effect of Access Site Choice on Acute Kidney Injury After Percutaneous Coronary Intervention.Am J Cardiol. 2017 Dec 15;120(12):2141-2145. doi: 10.1016/j.amjcard.2017.08.039. Epub 2017 Sep 20. Am J Cardiol. 2017. PMID: 29100589
-
Radial versus femoral access for percutaneous coronary intervention in patients with ST-segment elevation myocardial infarction: Trial sequential analysis.Am Heart J. 2020 Jun;224:98-104. doi: 10.1016/j.ahj.2020.03.014. Epub 2020 Mar 19. Am Heart J. 2020. PMID: 32361279 Review.
Cited by
-
Trans-radial versus trans-femoral approach for cerebral angiography: a meta-analysis of randomized controlled trials.Wideochir Inne Tech Maloinwazyjne. 2023 Jun;18(2):235-243. doi: 10.5114/wiitm.2022.123309. Epub 2022 Dec 22. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 37680739 Free PMC article.
References
-
- Mehran R., Aymong E., Nikolsky E., et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary interventionDevelopment and initial validation. Journal of the American College of Cardiology . 2004;44(7):1393–1399. doi: 10.1016/s0735-1097(04)01445-7. - DOI - PubMed
-
- Nusca A., Mangiacapra F., Sticchi A., et al. Usefulness of adding pre-procedural glycemia to the mehran score to enhance its ability to predict contrast-induced kidney injury in patients undergoing percutaneous coronary intervention development and validation of a predictive model. The American Journal of Cardiology . 2021;155:16–22. doi: 10.1016/j.amjcard.2021.06.014. - DOI - PubMed
-
- Valgimigli M., Frigoli E., Leonardi S., et al. Radial versus femoral access and bivalirudin versus unfractionated heparin in invasively managed patients with acute coronary syndrome (MATRIX): final 1-year results of a multicentre, randomised controlled trial. Lancet . 2018;392(10150):835–848. doi: 10.1016/S0140-6736(18)31714-8. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
