

Decline in Respiratory Functions in Hospitalized SARS-CoV-2 Infected Cancer Patients Following Cytotoxic Chemotherapy-An Additional Risk for Post-chemotherapy Complications
- PMID: 35360723
- PMCID: PMC8960442
- DOI: 10.3389/fmed.2022.835098
Decline in Respiratory Functions in Hospitalized SARS-CoV-2 Infected Cancer Patients Following Cytotoxic Chemotherapy-An Additional Risk for Post-chemotherapy Complications
Abstract
Background: Patients recovering from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection demonstrate impaired lung function and those requiring chemotherapy after recovering from SARS-CoV-2 infection have yet to be explored. In this study, we sought to investigate the possible pulmonary functional changes during and after administering chemotherapy in patients with prior SARS-CoV-2 infection.
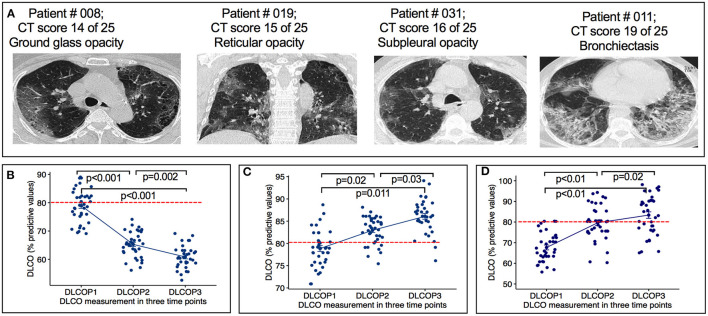
Methods: In this study, a total of 37 SARS-CoV-2 infected patients with cancer who were discharged from hospital and received subsequent cytotoxic chemotherapy were enrolled and prospectively followed-up. The following parameters were prospectively measured before (P1), after first chemotherapy cycle (P2), and 10 weeks after the end of chemotherapy (P3), to assess their impact on respiratory complications in terms of diffusion capacity of the lungs for carbon monoxide (DLCO), forced expiratory volume in 1-s (FEV1), forced vital capacity (FVC), 6-min walking distance (6MWD) test and levels of key inflammatory markers.
Results: All patients completed at least 2 cycles of chemotherapy without showing overt respiratory complications. Six patients (16%) complained about dyspnea during chemotherapy or at follow-up period. DLCO was significantly impaired during follow-up period [from P1 78 to P3 60% of predicted values; interquartile range (IQR) 55-89] and in 32 of 37 (86% of patients) from P1 to P2 (65% of predictive value; IQR 58-70; p < 0.001). Several patients experienced post-chemotherapy respiratory complications. As expected, all patients from control groups showed persistent improved pulmonary functions.
Conclusion: The risk of pulmonary impairments due to cytotoxic chemotherapy in prior SARS-CoV-2 infected patients is linked to the loss of DLCO. Accordingly, we recommend that for patients with cancer requiring chemotherapy after recovering from prior SARS-CoV-2 infection, pulmonary tests to be performed routinely before and during chemotherapy treatment to monitor the pulmonary performance.
Keywords: DLCO; HRCT (high resolution computed tomography); SARS-CoV-2; cancer; chemotherapy; pulmonary impairment.
Copyright © 2022 Al-Mozaini, Islam, Noman, Karim, Farhat, Yeger and Islam.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Betty R, Mark PC, Elizabeth MT, Nicola F, Ludovica G, Fidel AA, et al. Medium-term effects of SARS-CoV-2 infection on multiple vital organs, exercise capacity, cognition, quality of life and mental health, post-hospital discharge. EClinicalMedicine. (2021) 31:100683. 10.1016/j.eclinm.2020.100683 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous