

Transcutaneous Electrical Acupoint Stimulation Decreases the Incidence of Postoperative Nausea and Vomiting After Laparoscopic Non-gastrointestinal Surgery: A Multi-Center Randomized Controlled Trial
- PMID: 35360742
- PMCID: PMC8964119
- DOI: 10.3389/fmed.2022.766244
Transcutaneous Electrical Acupoint Stimulation Decreases the Incidence of Postoperative Nausea and Vomiting After Laparoscopic Non-gastrointestinal Surgery: A Multi-Center Randomized Controlled Trial
Abstract
Importance: Postoperative nausea and vomiting (PONV) gives patients a bad experience and negates their good recovery from surgery.
Objective: This trial aims to assess the preventive effectiveness of transcutaneous electrical acupoint stimulation (TEAS) on the incidence of PONV in high-risk surgical patients.
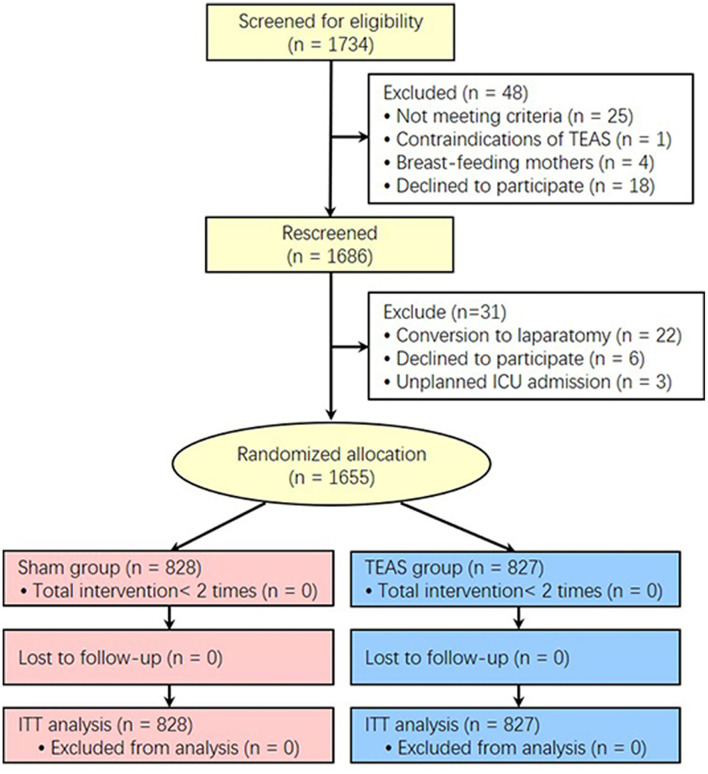
Design: The large sample size, multicenter, evaluator-blinded, and randomized controlled study was conducted between September 3, 2019 to February 6, 2021.
Setting: The 12 hospitals were from different Chinese provinces.
Participants: After obtaining ethics approval and written informed consent, 1,655 patients with Apfel score ≥ 3 points were enrolled for selective laparoscopic non-gastrointestinal surgery under general anesthesia.
Interventions: Patients were randomly allocated into the TEAS and Sham group with a 1:1 ratio. The TEAS group was stimulated on bilateral Neiguan and Zusanli acupoints after recovery from anesthesia on the surgical day and the next morning for 30 min, while the Sham group received an identical setting as TEAS but without currents delivered. Electronic patient self-reported scale was used to evaluate and record the occurrence of PONV.
Main outcomes and measures: Primary clinical end point is the incidence of PONV which was defined as at least one incidence of nausea, retching, or vomiting after operation within postoperative 24 h.
Results: Compared with the Sham treatment, the TEAS lowered the PONV incidence by 4.8% (29.4 vs. 34.2%, P = 0.036) and vomiting incidence by 7.4% (10.4 vs. 17.8%, P < 0.001). TEAS also lowered persistent nausea incidence and PONV scores and decreased PONV related complications and Quality of Recovery-40 scores (P < 0.05). TEAS lowered the 24 h PONV risk by 20% (OR, 0.80, 95% CI, 0.65 -0.98; P = 0.032), and lowered hazard ratio by 17% (HR, 0.83, 95% CI, 0.70-0.99; P = 0.035). Both TEAS and palonosetron were the independent PONV risk protective factors for 24 h PONV incidence and cumulative PONV incidence. The combination of TEAS and palonosetron was the most effective strategy to reduce the PONV incidence (P < 0.001).
Conclusions and relevance: TEAS attenuated the PONV incidence and severity in high-risk surgical patients and may be applied clinically as a complement therapy to prevent PONV.
Clinical trial registration: https://clinicaltrials.gov/ct2/show/NCT04043247, identifier: NCT04043247.
Keywords: antiemetic drugs; laparoscopic non-gastrointestinal surgery; nausea; transcutaneous electrical stimulation; vomiting.
Copyright © 2022 Gao, Zhang, Han, Wei, Fang, Zhang, Zhang, Wang, Zhou, Wang, Chen, Ni, Yang, Du, Wang, Liu, Li, Zhang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials