The British Orthopaedic Surgery Surveillance study: slipped capital femoral epiphysis: the epidemiology and two-year outcomes from a prospective cohort in Great Britain
- PMID: 35360942
- PMCID: PMC9020520
- DOI: 10.1302/0301-620X.104B4.BJJ-2021-1709.R1
The British Orthopaedic Surgery Surveillance study: slipped capital femoral epiphysis: the epidemiology and two-year outcomes from a prospective cohort in Great Britain
Abstract
Aims: The aim of this study was to inform the epidemiology and treatment of slipped capital femoral epiphysis (SCFE).
Methods: This was an anonymized comprehensive cohort study, with a nested consented cohort, following the the Idea, Development, Exploration, Assessment, Long-term study (IDEAL) framework. A total of 143 of 144 hospitals treating SCFE in Great Britain participated over an 18-month period. Patients were cross-checked against national administrative data and potential missing patients were identified. Clinician-reported outcomes were collected until two years. Patient-reported outcome measures (PROMs) were collected for a subset of participants.
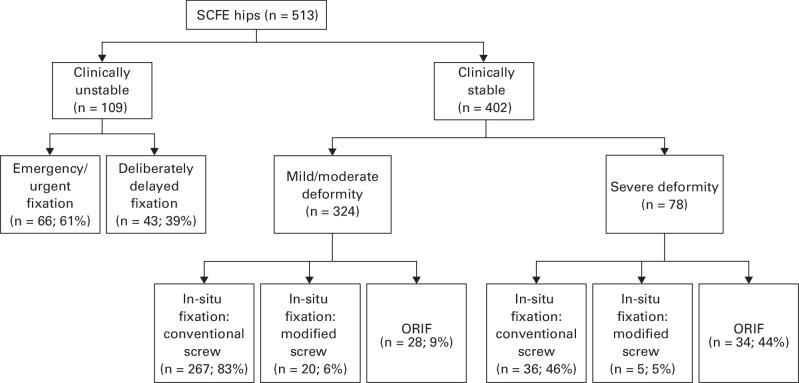
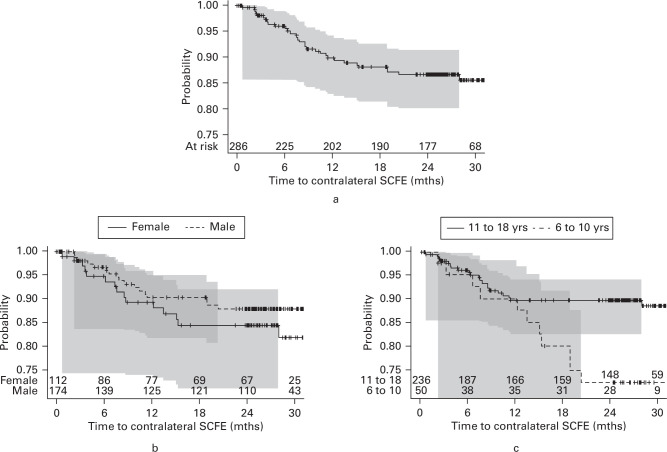
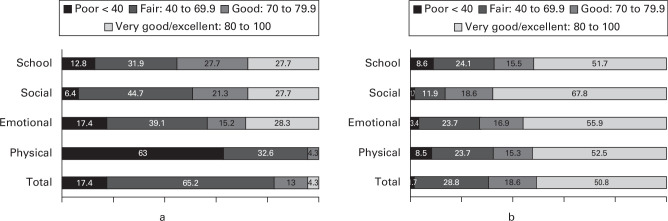
Results: A total of 486 children (513 hips) were newly affected, with a median of two patients (interquartile range 0 to 4) per hospital. The annual incidence was 3.34 (95% confidence interval (CI) 3.01 to 3.67) per 100,000 six- to 18-year-olds. Time to diagnosis in stable disease was increased in severe deformity. There was considerable variation in surgical strategy among those unable to walk at diagnosis (66 urgent surgery vs 43 surgery after interval delay), those with severe radiological deformity (34 fixation with deformity correction vs 36 without correction) and those with unaffected opposite hips (120 prophylactic fixation vs 286 no fixation). Independent risk factors for avascular necrosis (AVN) were the inability of the child to walk at presentation to hospital (adjusted odds ratio (aOR) 4.4 (95% CI 1.7 to 11.4)) and surgical technique of open reduction and internal fixation (aOR 7.5 (95% CI 2.4 to 23.2)). Overall, 33 unaffected untreated opposite hips (11.5%) were treated for SCFE by two-year follow-up. Age was the only independent risk factor for contralateral SCFE, with age under 12.5 years the optimal cut-off to define 'at risk'. Of hips treated with prophylactic fixation, none had SCFE, though complications included femoral fracture, AVN, and revision surgery. PROMs demonstrated the marked impact on quality of life on the child because of SCFE.
Conclusion: The experience of individual hospitals is limited and mechanisms to consolidate learning may enhance care. Diagnostic delays were common and radiological severity worsened with increasing time to diagnosis. There was unexplained variation in treatment, some of which exposes children to significant risks that should be evaluated through randomized controlled trials. Cite this article: Bone Joint J 2022;104-B(4):519-528.
Keywords: Avascular necrosis; BOSS; Cohort study; Epidemiology; Incidence; Patient-reported outcome measures (PROMs); SCFE; SUFE; Slipped capital femoral epiphysis; Slipped capital femoral epiphysis (SCFE); Slipped upper femoral epiphysis; avascular necrosis; clinicians; deformity; hip(s); open reduction and internal fixation; orthopaedic surgery; prophylactic fixation; randomized controlled trials.
Figures