

Risk factors for placental malaria, sulfadoxine-pyrimethamine doses, and birth outcomes in a rural to urban prospective cohort study on the Bandiagara Escarpment and Bamako, Mali
- PMID: 35361195
- PMCID: PMC8974163
- DOI: 10.1186/s12936-022-04125-6
Risk factors for placental malaria, sulfadoxine-pyrimethamine doses, and birth outcomes in a rural to urban prospective cohort study on the Bandiagara Escarpment and Bamako, Mali
Abstract
Background: Malaria in Mali remains a primary cause of morbidity and mortality, with women at high risk during pregnancy for placental malaria (PM). Risk for PM and its association with birth outcomes was evaluated in a rural to urban longitudinal cohort on the Bandiagara Escarpment and the District of Bamako.
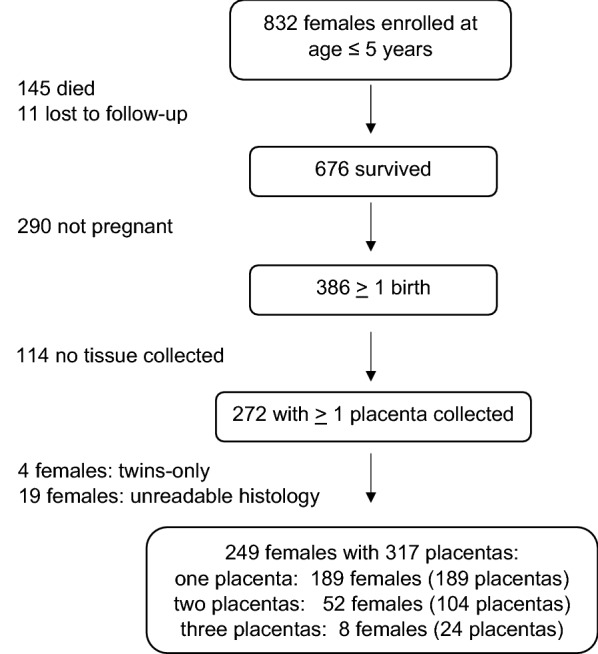
Methods: Placental samples (N = 317) were collected from 249 mothers who were participants in a prospective cohort study directed by BIS in the years 2011 to 2019. A placental pathologist and research assistant evaluated the samples by histology in blinded fashion to assess PM infection stage and parasite density. Generalized estimating equations (GEE) were used to model the odds of PM infection.
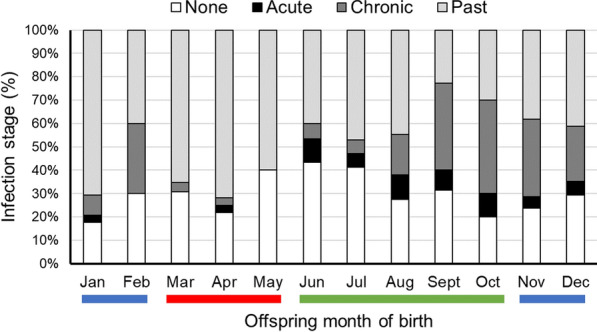
Results: In a multivariable model, pregnancies in Bamako, beyond secondary education, births in the rainy season (instead of the hot dry season), and births to women who had ≥ 3 doses of sulfadoxine-pyrimethamine (SP) instead of no doses were associated with reduced odds of experiencing PM (active and past infections combined). Births in later years of the study were strongly associated with reduced odds of PM. Maternal age, which was positively associated with offspring year of birth, was significant as a predictor of PM only if offspring year of birth was omitted from the model. Gravidity was positively associated with both maternal age and offspring year of birth such that if either variable was included in the model, then gravidity was no longer significant. However, if maternal age or year of offspring birth were not adjusted for, then the odds of PM were nearly two-fold higher in primigravida compared to multigravida. Birth outcomes improved (+ 285 g birth weight, + 2 cm birth length, + 75 g placental weight) for women who had ≥ 3 doses of SP compared to no doses, but no difference was detected in birth weight or length for women who had 2 instead of ≥ 3 SP doses. However, at 2 instead of ≥ 3 doses placentas were 36 g lighter and the odds of low birth weight (< 2500 g) were 14% higher. Severe parasite densities (> 10% erythrocytes infected) were significantly associated with decreases in birth weight, birth length, and placental weight, as were chronic PM infections. The women who received no SP during pregnancy (7% of the study total) were younger and lacked primary school education. The women who received ≥ 3 doses of SP came from more affluent families.
Conclusions: Women who received no doses of SP during pregnancy experienced the most disadvantageous birth outcomes in both Bamako and on the Bandiagara Escarpment. Such women tended to be younger and to have had no primary school education. Targeting such women for antenatal care, which is the setting in which SP is most commonly administered in Mali, will have a more positive impact on public health than focusing on the increment from two to three doses of SP, although that increment is also desirable.
Keywords: Birth seasonality; Birth weight; Cohort; Histology; IPTp; Malaria; Maternal education; Placenta; Pregnancy; Sulfadoxine-pyrimethamine.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that we have no competing interests.
Figures
Similar articles
-
Assessing malaria burden during pregnancy in Mali.Acta Trop. 2007 May;102(2):106-12. doi: 10.1016/j.actatropica.2007.04.005. Epub 2007 Apr 21. Acta Trop. 2007. PMID: 17543872
-
Superiority of 3 over 2 doses of intermittent preventive treatment with sulfadoxine-pyrimethamine for the prevention of malaria during pregnancy in mali: a randomized controlled trial.Clin Infect Dis. 2011 Aug 1;53(3):215-23. doi: 10.1093/cid/cir374. Clin Infect Dis. 2011. PMID: 21765069 Clinical Trial.
-
Coverage and effectiveness of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) on adverse pregnancy outcomes in the Mount Cameroon area, South West Cameroon.Malar J. 2020 Mar 2;19(1):100. doi: 10.1186/s12936-020-03155-2. Malar J. 2020. PMID: 32122339 Free PMC article.
-
Safety and toxicity of sulfadoxine/pyrimethamine: implications for malaria prevention in pregnancy using intermittent preventive treatment.Drug Saf. 2007;30(6):481-501. doi: 10.2165/00002018-200730060-00003. Drug Saf. 2007. PMID: 17536875 Review.
-
Impact of Malaria in Pregnancy on Risk of Malaria in Young Children: Systematic Review and Meta-Analyses.J Infect Dis. 2020 Jul 23;222(4):538-550. doi: 10.1093/infdis/jiaa139. J Infect Dis. 2020. PMID: 32219317 Free PMC article.
Cited by
-
Placental Malaria and Its Relationship with Neonatal Birth Weight among Primigravidae: An Analytical Cross-sectional Study.Explor Res Hypothesis Med. 2024;9(3):181-191. doi: 10.14218/erhm.2023.00015. Epub 2024 Jun 20. Explor Res Hypothesis Med. 2024. PMID: 39267914 Free PMC article.
-
Drug-Drug Interaction Between Dihydroartemisinin-Piperaquine and Sulfadoxine-Pyrimethamine During Malaria Chemoprevention in Pregnant Women.Clin Pharmacol Ther. 2025 Feb;117(2):506-514. doi: 10.1002/cpt.3471. Epub 2024 Oct 14. Clin Pharmacol Ther. 2025. PMID: 39402742 Clinical Trial.
-
What are the pathways between poverty and malaria in sub-Saharan Africa? A systematic review of mediation studies.Infect Dis Poverty. 2023 Jun 8;12(1):58. doi: 10.1186/s40249-023-01110-2. Infect Dis Poverty. 2023. PMID: 37291664 Free PMC article.
-
Level of and factors associated with optimal uptake of intermittent preventive treatment for malaria in pregnancy at private-not-for-profit health facilities in Kasese district.PLOS Glob Public Health. 2024 Apr 3;4(4):e0002622. doi: 10.1371/journal.pgph.0002622. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 38569001 Free PMC article.
References
-
- WHO. World Malaria Report: 20 years of global progress and challenges. Geneva, World Health Organization, 2020.
-
- Guyatt HL, Snow RW. The epidemiology and burden of Plasmodium falciparum-related anemia among pregnant women in sub-Saharan Africa. Am J Trop Med Hyg. 2001;64:36–44. - PubMed
-
- WHO . World malaria report 2019. Geneva: World Health Organization; 2019.
-
- Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Glob Health. 2013;1:e16–25. - PMC - PubMed
MeSH terms
Substances
Grants and funding
- R01 HD088521/HD/NICHD NIH HHS/United States
- NSF BCS-1354814/National Science Foundation
- 52269/John Templeton Foundation
- R01HD088521/Eunice Kennedy Shriver National Institute of Child Health and Human Development
- R21HD077465/Eunice Kennedy Shriver National Institute of Child Health and Human Development
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
