

CAR race to cancer immunotherapy: from CAR T, CAR NK to CAR macrophage therapy
- PMID: 35361234
- PMCID: PMC8969382
- DOI: 10.1186/s13046-022-02327-z
CAR race to cancer immunotherapy: from CAR T, CAR NK to CAR macrophage therapy
Abstract
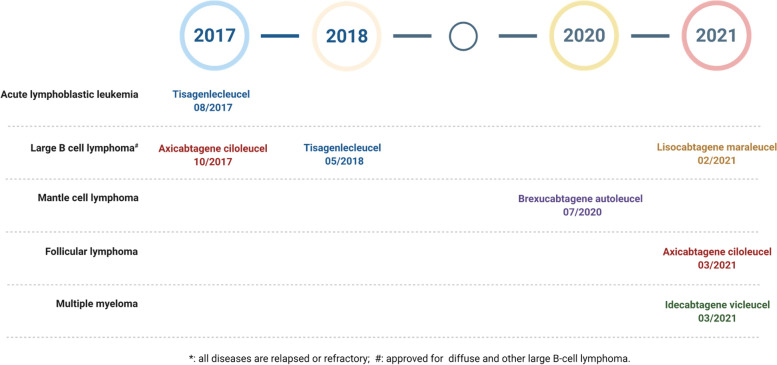
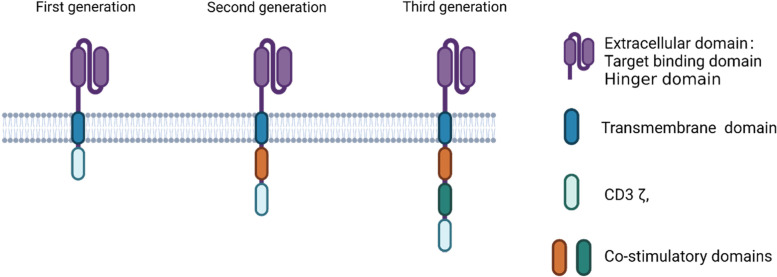
Adoptive cell therapy with chimeric antigen receptor (CAR) immunotherapy has made tremendous progress with five CAR T therapies approved by the US Food and Drug Administration for hematological malignancies. However, CAR immunotherapy in solid tumors lags significantly behind. Some of the major hurdles for CAR immunotherapy in solid tumors include CAR T cell manufacturing, lack of tumor-specific antigens, inefficient CAR T cell trafficking and infiltration into tumor sites, immunosuppressive tumor microenvironment (TME), therapy-associated toxicity, and antigen escape. CAR Natural Killer (NK) cells have several advantages over CAR T cells as the NK cells can be manufactured from pre-existing cell lines or allogeneic NK cells with unmatched major histocompatibility complex (MHC); can kill cancer cells through both CAR-dependent and CAR-independent pathways; and have less toxicity, especially cytokine-release syndrome and neurotoxicity. At least one clinical trial showed the efficacy and tolerability of CAR NK cell therapy. Macrophages can efficiently infiltrate into tumors, are major immune regulators and abundantly present in TME. The immunosuppressive M2 macrophages are at least as efficient as the proinflammatory M1 macrophages in phagocytosis of target cells; and M2 macrophages can be induced to differentiate to the M1 phenotype. Consequently, there is significant interest in developing CAR macrophages for cancer immunotherapy to overcome some major hurdles associated with CAR T/NK therapy, especially in solid tumors. Nevertheless, both CAR NK and CAR macrophages have their own limitations. This comprehensive review article will discuss the current status and the major hurdles associated with CAR T and CAR NK therapy, followed by the structure and cutting-edge research of developing CAR macrophages as cancer-specific phagocytes, antigen presenters, immunostimulators, and TME modifiers.
Keywords: Adoptive cell transfer; CAR NK cells; CAR T therapy; CAR macrophage; Chimeric antigen receptor (CAR); Cytokine release syndrome; Immunotherapy; Tumor microenvironment.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- U.S. FDA Approves Yescarta for Relapsed or Refractory Follicular Lymphoma After Two or More Lines of Systemic Therapy [https://www.drugs.com/newdrugs/u-s-fda-approves-yescarta-relapsed-refrac...]
-
- Munshi NC, Anderson LD, Jr, Shah N, Madduri D, Berdeja J, Lonial S, et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. N Engl J Med. 2021;384(8):705–716. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
