

Outcomes Associated With Peripheral Artery Disease in Myocardial Infarction With Cardiogenic Shock
- PMID: 35361344
- PMCID: PMC9172933
- DOI: 10.1016/j.jacc.2022.01.037
Outcomes Associated With Peripheral Artery Disease in Myocardial Infarction With Cardiogenic Shock
Abstract
Background: Mortality rates for patients presenting with acute myocardial infarction (AMI) and cardiogenic shock (CS) remain high despite advances in revascularization strategies and mechanical circulatory support (MCS) devices.
Objectives: This study sought to elucidate the association between comorbid lower extremity peripheral artery disease (PAD) and outcomes in CS and AMI.
Methods: PAD status was defined in Medicare beneficiaries hospitalized with CS and AMI from October 1, 2015 to June 30, 2018. Primary outcomes ascertained through December 31, 2018 included in- and out-of-hospital mortality. Secondary outcomes included bleeding, amputation, stroke, and lower extremity revascularization. Multivariable regression models with adjustment for confounders were used to estimate risk. Subgroup analyses included patients treated with MCS and those who underwent coronary revascularization.
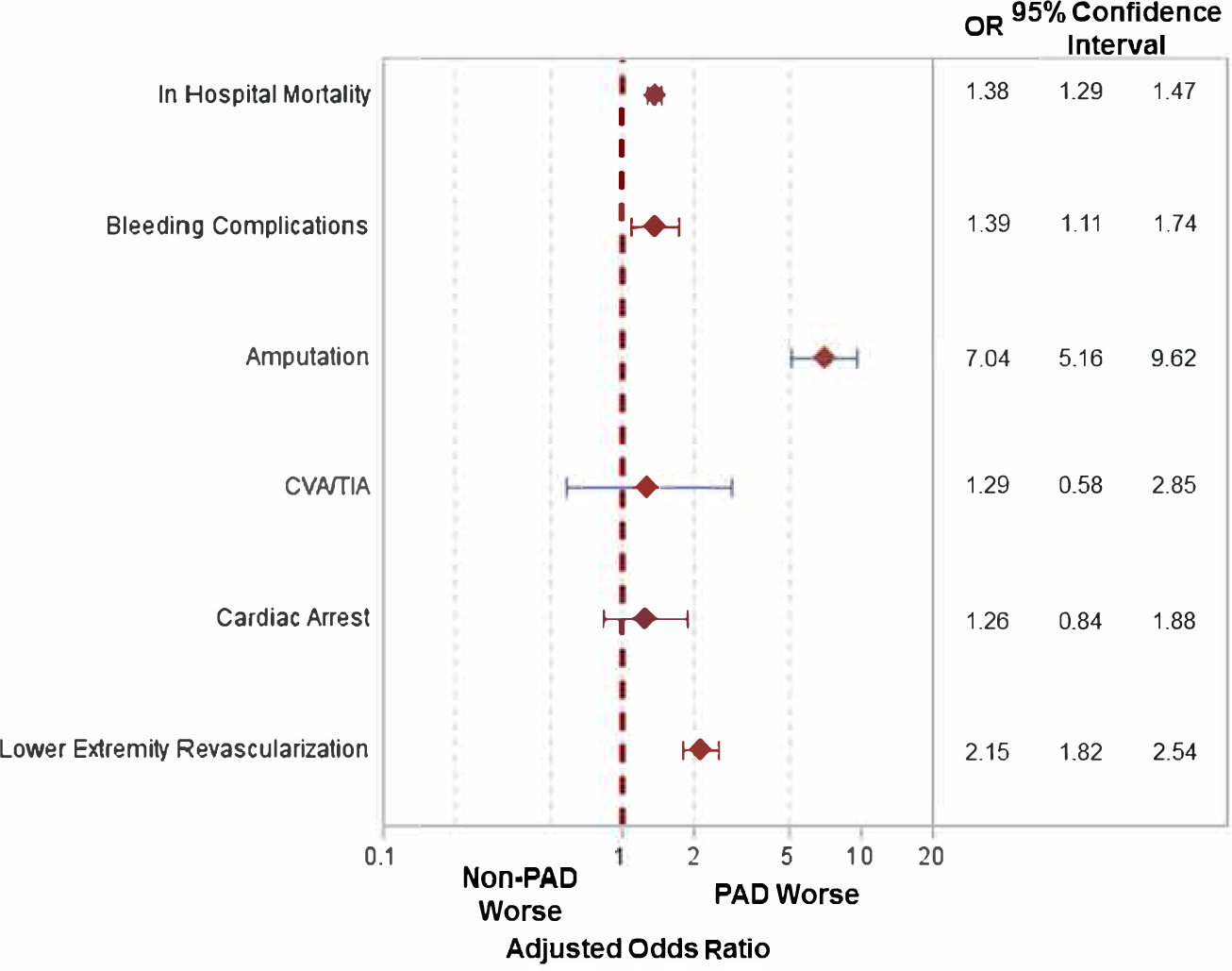
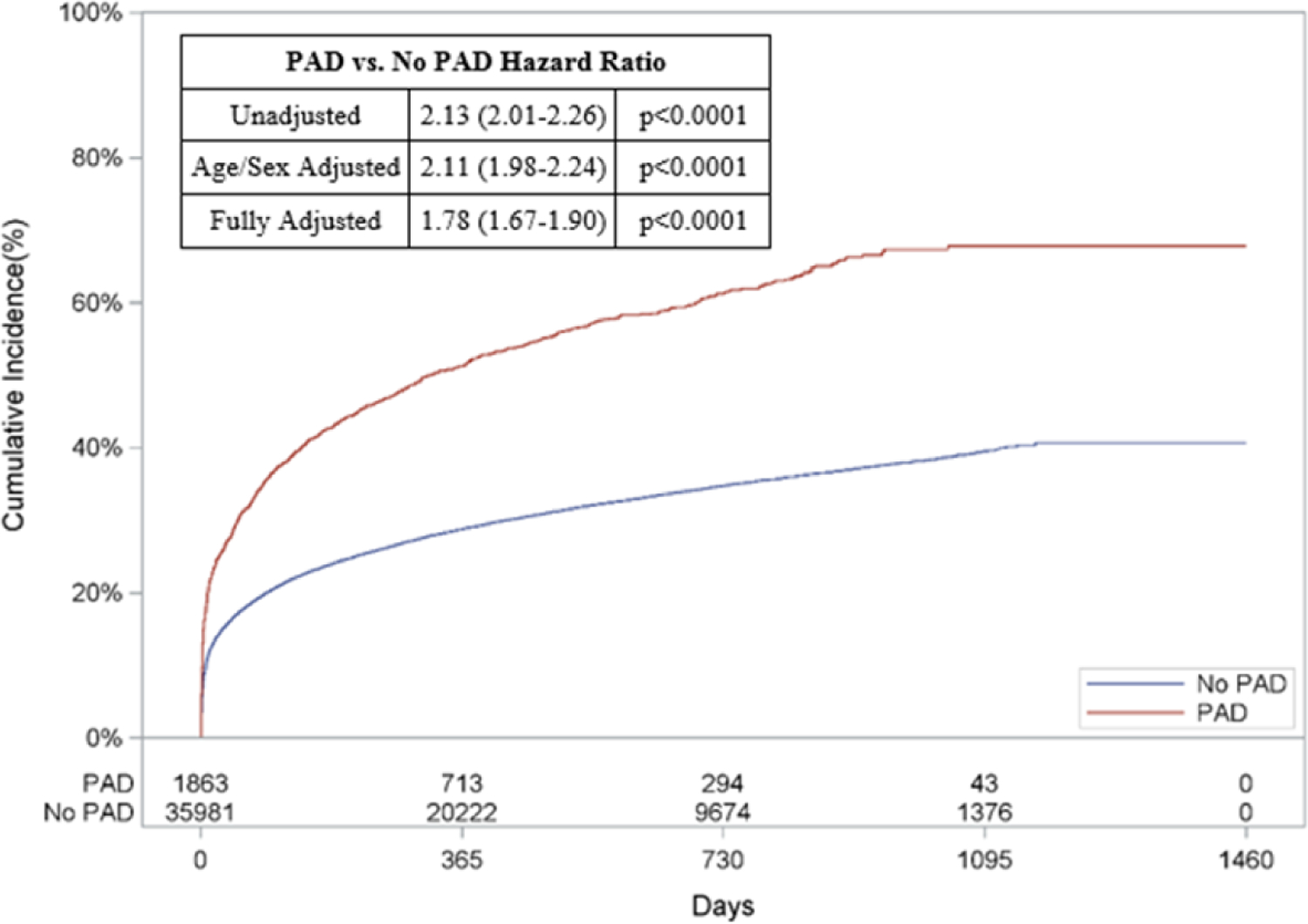
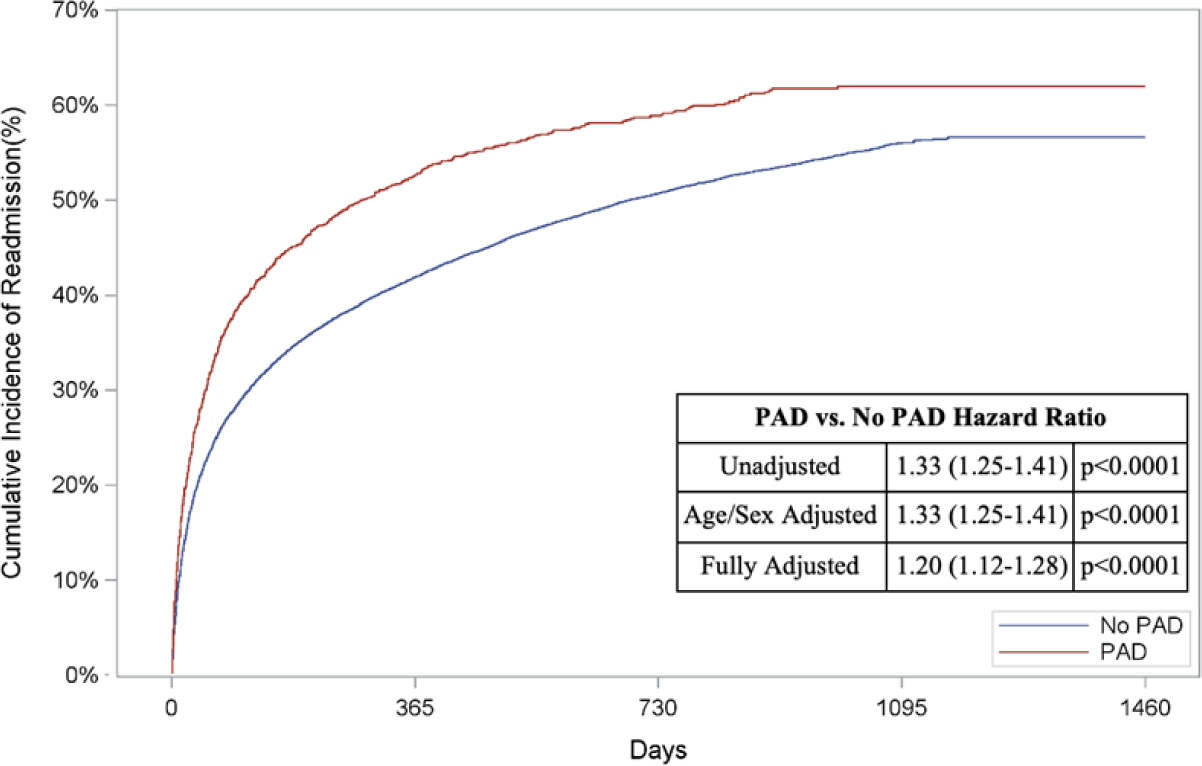
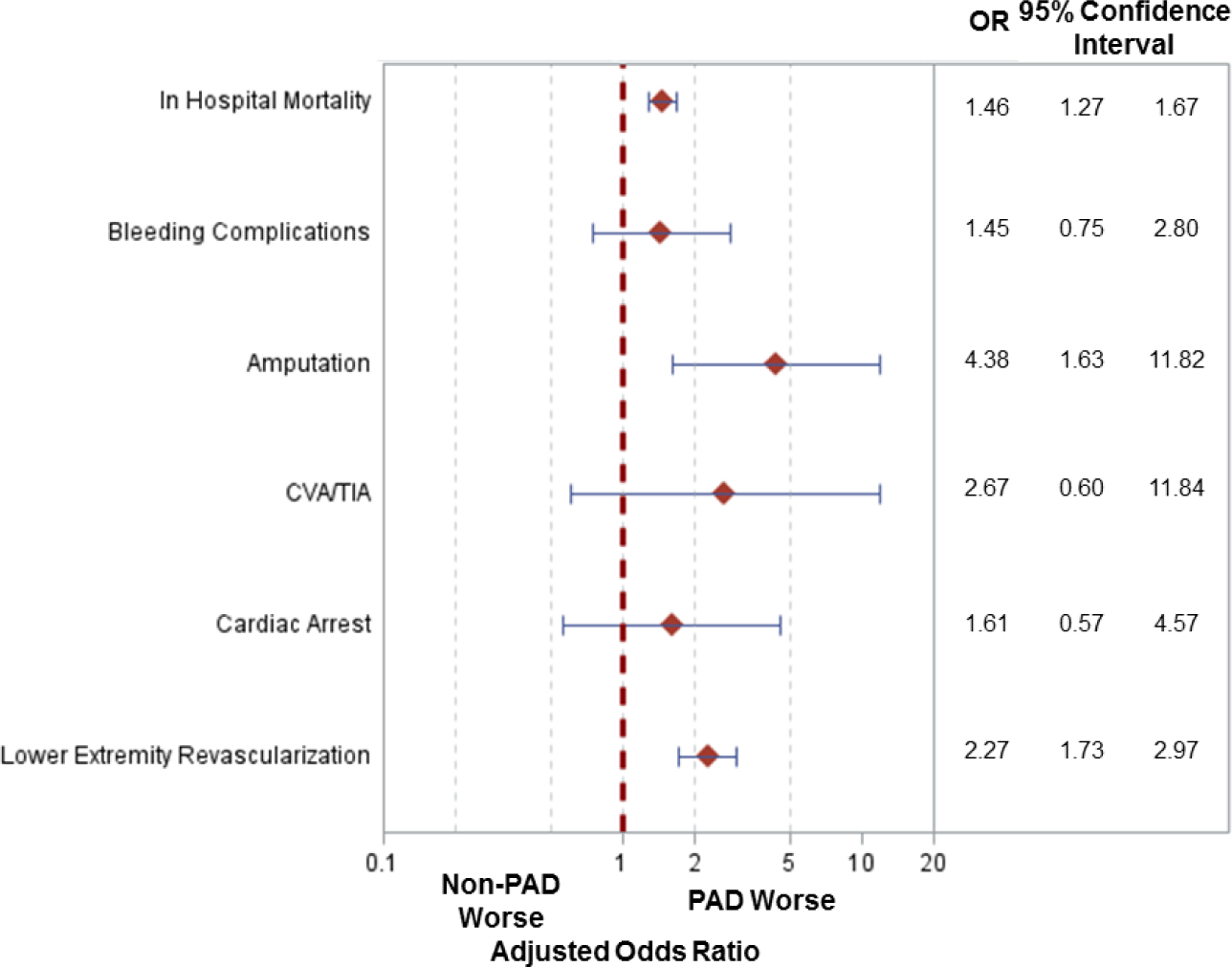
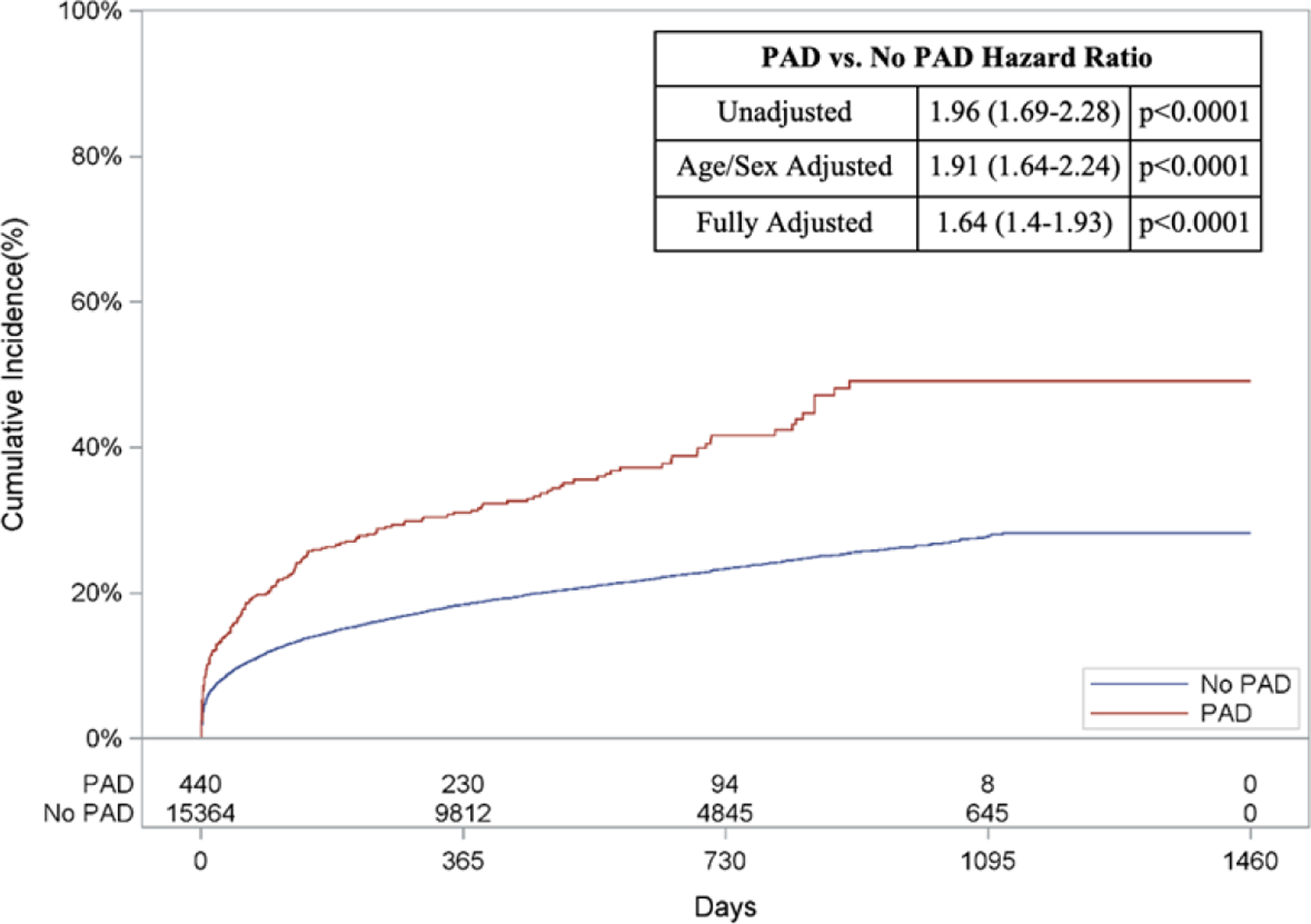
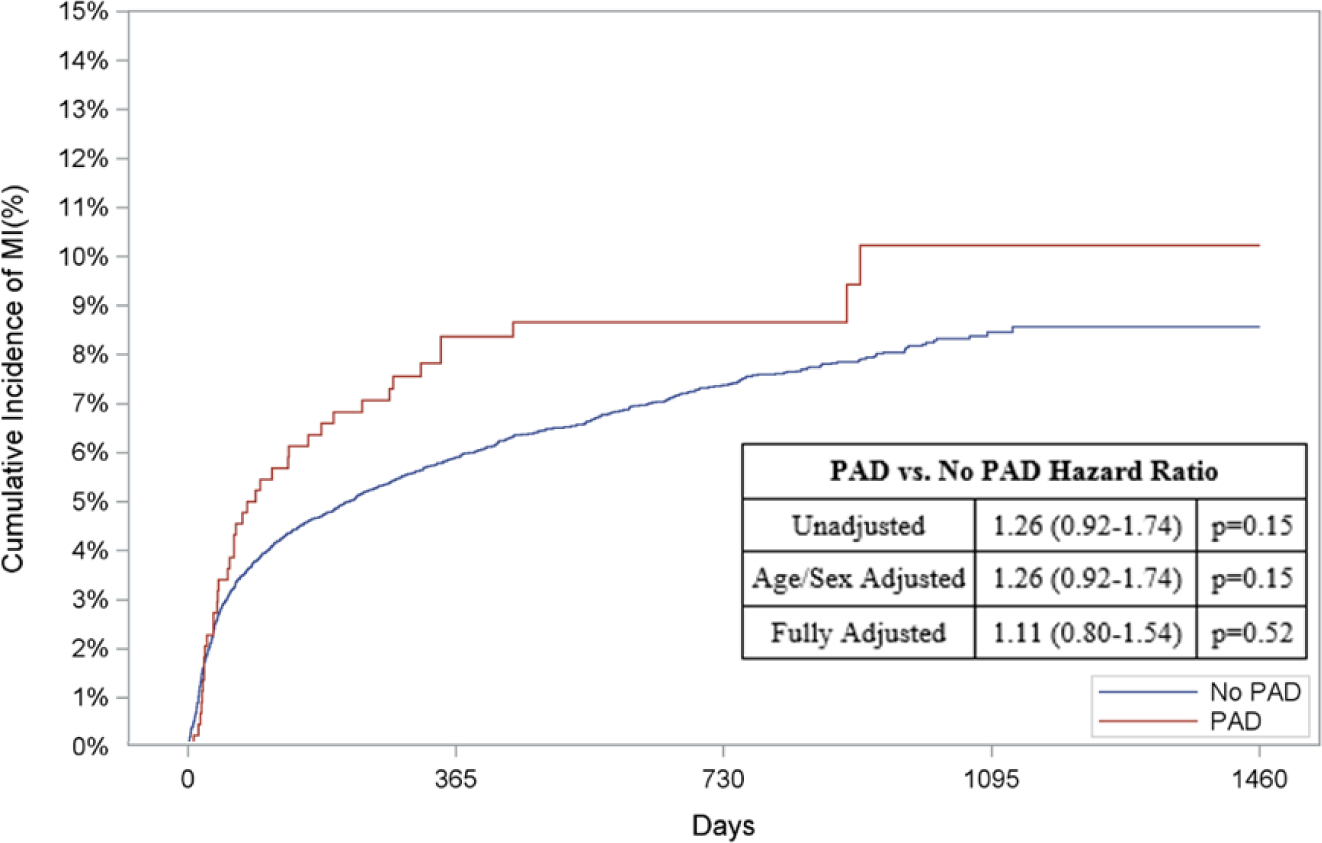
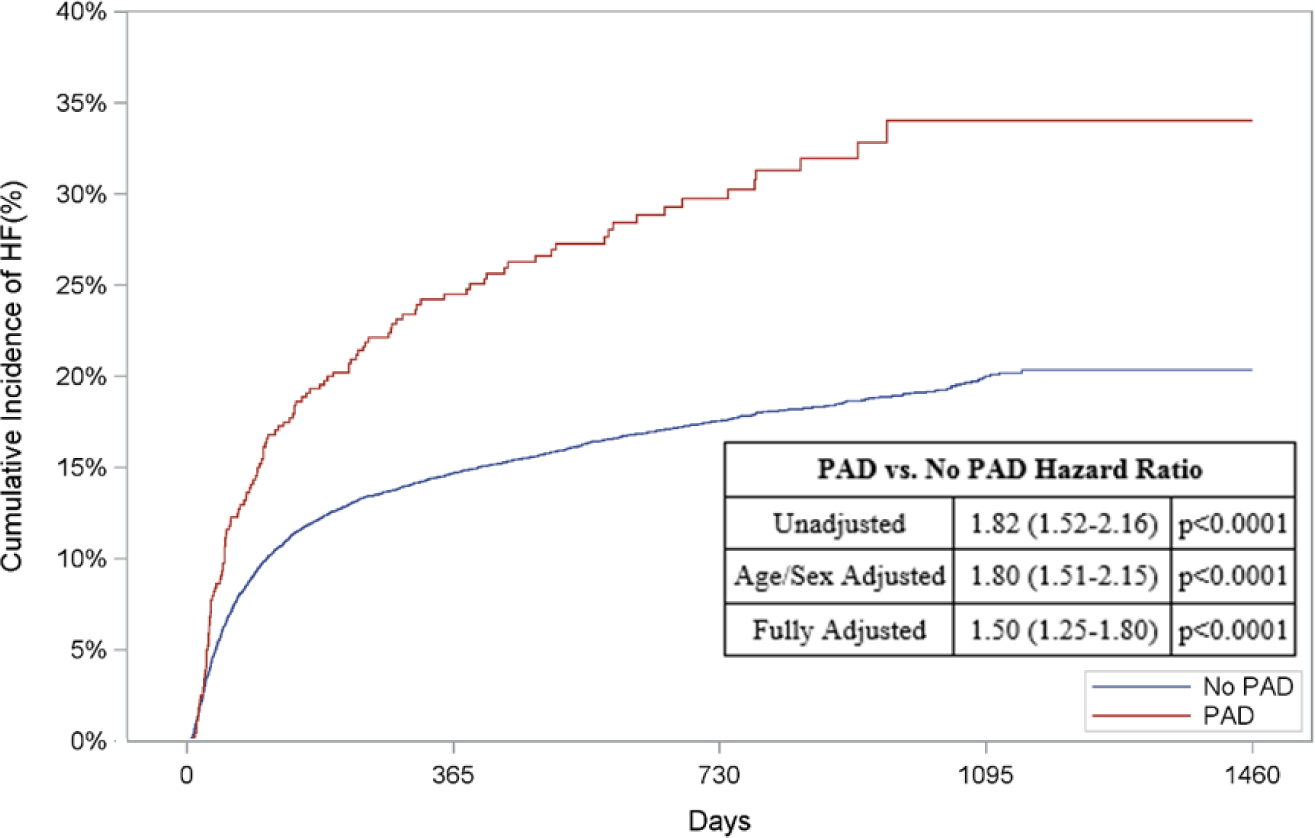
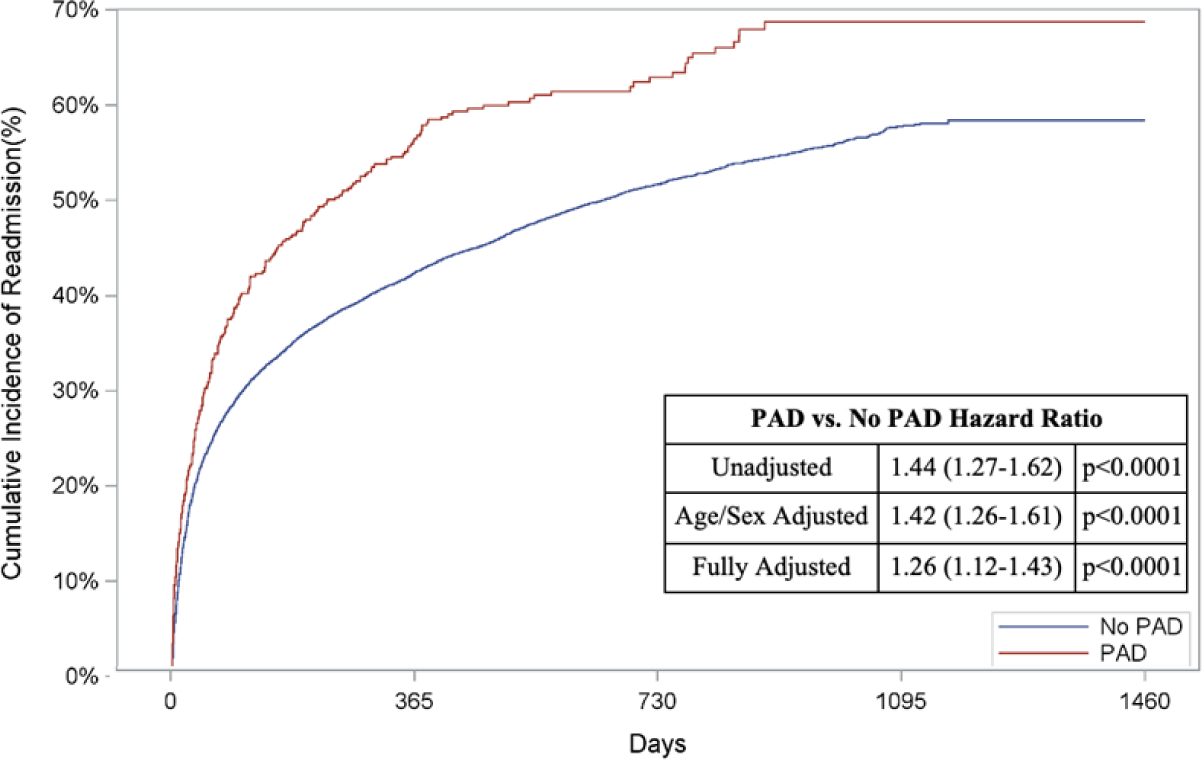
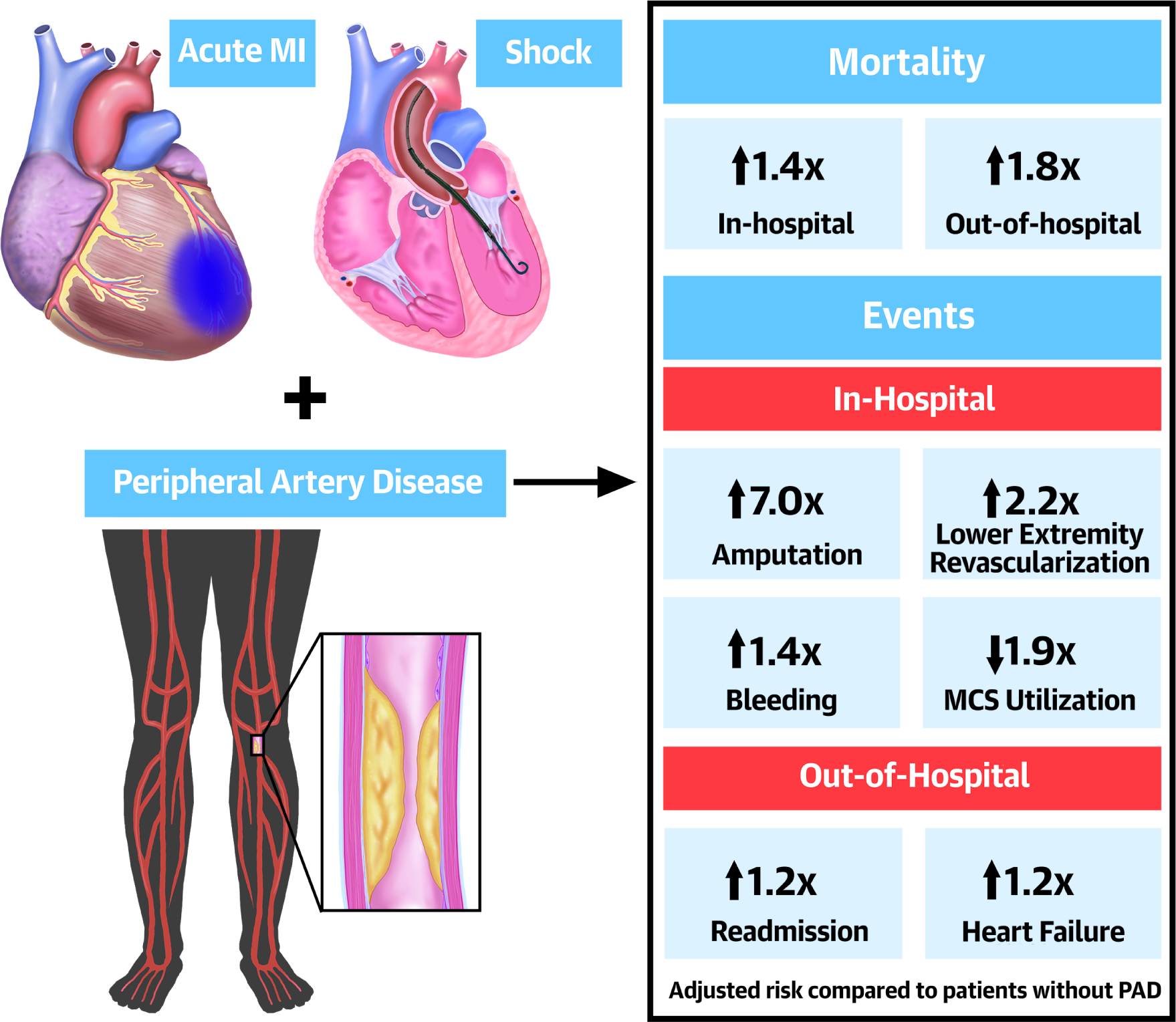
Results: Among 71,690 patients, 5.9% (N = 4,259) had PAD. Mean age was 77.8 ± 7.9 years, 58.7% were male, and 84.3% were White. Cumulative in-hospital mortality was 47.2%, with greater risk among those with PAD (56.3% vs 46.6% without PAD; adjusted OR: 1.50; 95% CI: 1.40-1.59). PAD patients also had greater risk of in-hospital amputation (1.6% vs 0.2%; adjusted OR: 7.0; 95% CI: 5.26-9.37) and out-of-hospital mortality (67.9% vs 40.7%; adjusted HR: 1.78; 95% CI: 1.67-1.90). MCS was less frequently utilized in PAD patients (21.5% vs 38.6% without PAD; P < 0.001) and was associated with higher mortality, need for lower extremity revascularization, and amputation risk. Findings were consistent in patients who underwent coronary revascularization.
Conclusions: Among patients presenting with AMI and CS, PAD was associated with worse limb outcomes and survival. In addition to lower MCS utilization rates, those with PAD who received MCS had increased mortality, lower extremity revascularization, and amputation rates.
Keywords: cardiogenic shock; coronary artery bypass grafting; mechanical circulatory support; myocardial infarction; percutaneous coronary intervention; peripheral artery disease.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Mihatov has been funded by National Institutes of Health (NIH) grant T32HL007208. Dr Kirtane has received funding for research grants, speaking engagements and/or consulting paid to his institutions from Medtronic, Boston Scientific, Abbott Vascular, Abiomed, CSI, CathWorks, Siemens, Philips, and ReCor Medical; and has received personal fees for travel expenses/meals from Medtronic, Boston Scientific, Abbott Vascular, Abiomed, CSI, CathWorks, Siemens, Philips, ReCor Medical, Chiesi, OpSens, Zoll, and Regeneron. Dr Parikh has received institutional research support from Abbott Vascular, TriReme Medical, SurModics, and Shockwave Medical; is an advisory board member for Abbott Vascular, Boston Scientific, Cardinal Health, Medtronic, Janssen, CSI, and Philips; and receives honoraria from Abiomed and Terumo. Dr Rosenfield has served as a consultant to or on the scientific advisory board for Access Vascular, Althea Medical, Angiodynamics, BMS-Pfizer, Boston Scientific, Contego, Janssen, InspireMD, Magneto, Mayo Clinic, Neptune Medical, Philips, Summa Therapeutics, Surmodics, Thrombolex, Terumo, and Truvic; has received institutional grants from the NIH, Philips, Intact Vascular, and Boston Scientific; has equity in Accolade, Access Vascular, Althea Medical, Contego, Cruzar Systems, Embolitech, Endospan, Eximo, InspireMG, JanaCare, Magneto, Micell, Neptune Medical, Orchestra, PQ Bypass, Prosomnus, Shockwave, Summa Therapeutics, Thrombolex, Truvic, and Valcare; and serves as a board member for the National PERT Consortium. Dr Yeh has served on scientific advisory boards, consulted for, and received research support from Abbott Vascular, AstraZeneca, Boston Scientific, and Medtronic; and receives funding from the National Heart, Lung, and Blood Institute grant R01HL136708 and the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology. Dr Secemsky has received consulting and/or speaking fees from Bard, Cook Medical, CSI, Medtronic, and Phillips; and receives research support from NIH/NHLBI K23HL150290, Food & Drug Administration, Harvard Medical School’s Shore Faculty Development Award, AstraZeneca, Bard, Boston Scientific, Cook Medical, CSI, Laminate Medical, Medtronic, and Philips. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Peripheral Artery Disease: The New and Old Silent Killer.J Am Coll Cardiol. 2022 Apr 5;79(13):1236-1238. doi: 10.1016/j.jacc.2022.02.006. J Am Coll Cardiol. 2022. PMID: 35361345 No abstract available.
Similar articles
-
Inpatient Outcomes for Patients With Peripheral Artery Disease Hospitalized for Acute Myocardial Infarction.J Am Heart Assoc. 2025 Jun 17;14(12):e040526. doi: 10.1161/JAHA.124.040526. Epub 2025 Jun 11. J Am Heart Assoc. 2025. PMID: 40497502 Free PMC article.
-
Revascularization Practices and Outcomes in Patients With Multivessel Coronary Artery Disease Who Presented With Acute Myocardial Infarction and Cardiogenic Shock in the US, 2009-2018.JAMA Intern Med. 2020 Oct 1;180(10):1317-1327. doi: 10.1001/jamainternmed.2020.3276. JAMA Intern Med. 2020. PMID: 32833024 Free PMC article.
-
Trends in mechanical circulatory support use and hospital mortality among patients with acute myocardial infarction and non-infarction related cardiogenic shock in the United States.Clin Res Cardiol. 2018 Apr;107(4):287-303. doi: 10.1007/s00392-017-1182-2. Epub 2017 Nov 13. Clin Res Cardiol. 2018. PMID: 29134345
-
Characteristics and Outcomes of Early vs Late Initiation of Mechanical Circulatory Support in Non-Acute Myocardial Infarction related Cardiogenic Shock: An Analysis of the National Inpatient Sample Database.Curr Probl Cardiol. 2023 May;48(5):101584. doi: 10.1016/j.cpcardiol.2023.101584. Epub 2023 Jan 13. Curr Probl Cardiol. 2023. PMID: 36642353 Review.
-
Current clinical management of acute myocardial infarction complicated by cardiogenic shock.Expert Rev Cardiovasc Ther. 2021 Jan;19(1):41-46. doi: 10.1080/14779072.2021.1854733. Epub 2021 Jan 19. Expert Rev Cardiovasc Ther. 2021. PMID: 33289436 Review.
Cited by
-
Position Statement on Vascular Access Safety for Percutaneous Devices in AMI Complicated by Cardiogenic Shock.JACC Cardiovasc Interv. 2022 Oct 24;15(20):2003-2019. doi: 10.1016/j.jcin.2022.08.041. JACC Cardiovasc Interv. 2022. PMID: 36265932 Free PMC article. Review.
-
Nomogram prediction model for the risk of intracranial hemorrhagic transformation after intravenous thrombolysis in patients with acute ischemic stroke.Front Neurol. 2024 Mar 7;15:1361035. doi: 10.3389/fneur.2024.1361035. eCollection 2024. Front Neurol. 2024. PMID: 38515444 Free PMC article.
-
Inpatient Outcomes for Patients With Peripheral Artery Disease Hospitalized for Acute Myocardial Infarction.J Am Heart Assoc. 2025 Jun 17;14(12):e040526. doi: 10.1161/JAHA.124.040526. Epub 2025 Jun 11. J Am Heart Assoc. 2025. PMID: 40497502 Free PMC article.
-
Mechanisms and Therapeutic Strategies for Myocardial Ischemia-Reperfusion Injury in Diabetic States.ACS Pharmacol Transl Sci. 2024 Nov 1;7(12):3691-3717. doi: 10.1021/acsptsci.4c00272. eCollection 2024 Dec 13. ACS Pharmacol Transl Sci. 2024. PMID: 39698288 Review.
-
Comparative analysis of cardiogenic shock outcomes in acute myocardial infarction with polyvascular disease.Am Heart J Plus. 2024 Aug 31;46:100452. doi: 10.1016/j.ahjo.2024.100452. eCollection 2024 Oct. Am Heart J Plus. 2024. PMID: 39319104 Free PMC article.
References
-
- Goldberg RJ, Makam RCP, Yarzebski J, McManus DD, Lessard D, Gore JM. Decade-Long Trends (2001–2011) in the Incidence and Hospital Death Rates Associated with the In-Hospital Development of Cardiogenic Shock after Acute Myocardial Infarction. Circulation: Cardiovascular Quality and Outcomes 2016;9:117–125. - PMC - PubMed
-
- Aissaoui N, Puymirat E, Tabone X et al. Improved outcome of cardiogenic shock at the acute stage of myocardial infarction: a report from the USIK 1995, USIC 2000, and FAST-MI French nationwide registries. Eur Heart J 2012;33:2535–2543. - PubMed
-
- Poredos P, Jug B. The prevalence of peripheral arterial disease in high risk subjects and coronary or cerebrovascular patients. Angiology 2007;58:309–15. - PubMed
-
- Jeremias A, Gruberg L, Patel J, Connors G, Brown DL. Effect of peripheral arterial disease on in-hospital outcomes after primary percutaneous coronary intervention for acute myocardial infarction. Am J Cardiol 2010;105:1268–1271. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
