

Mechanical Left Ventricular Unloading in Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation
- PMID: 35361346
- PMCID: PMC9187498
- DOI: 10.1016/j.jacc.2022.01.032
Mechanical Left Ventricular Unloading in Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation
Abstract
Background: Venoarterial extracorporeal membrane oxygenation (VA-ECMO) increases left ventricular (LV) afterload, potentially provoking LV distention and impairing recovery. LV mechanical unloading (MU) with intra-aortic balloon pump (IABP) or percutaneous ventricular assist device (pVAD) can prevent LV distension, potentially at the risk of more complications, and net clinical benefit remains uncertain.
Objectives: This study aims to determine the association between MU and outcomes for patients undergoing VA-ECMO.
Methods: The authors queried the Extracorporeal Life Support Organization registry for adults receiving peripheral VA-ECMO from 2010 to 2019 and stratified them by MU with IABP or pVAD. The primary outcome was in-hospital mortality; secondary outcomes included on-support mortality and complications during VA-ECMO.
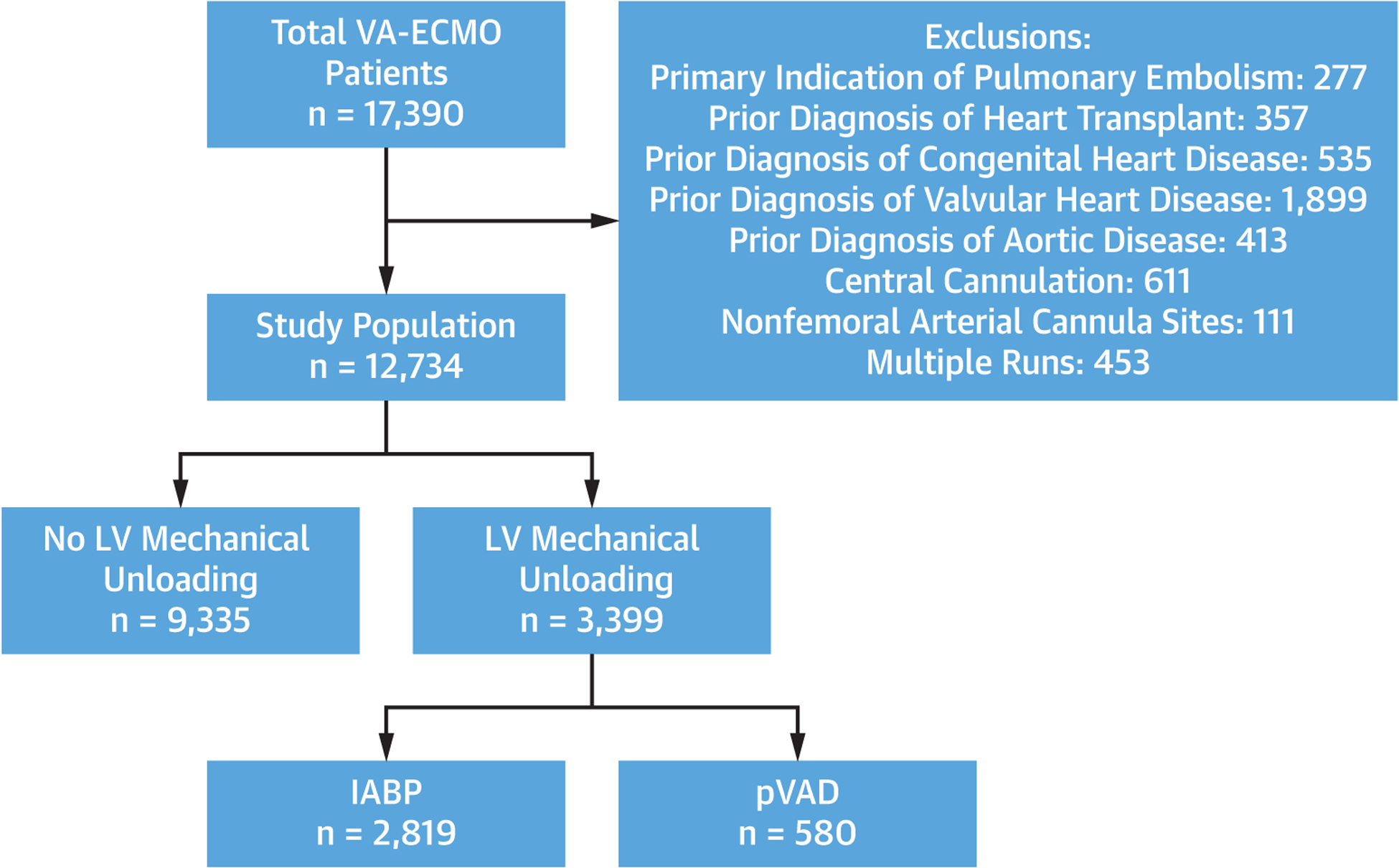
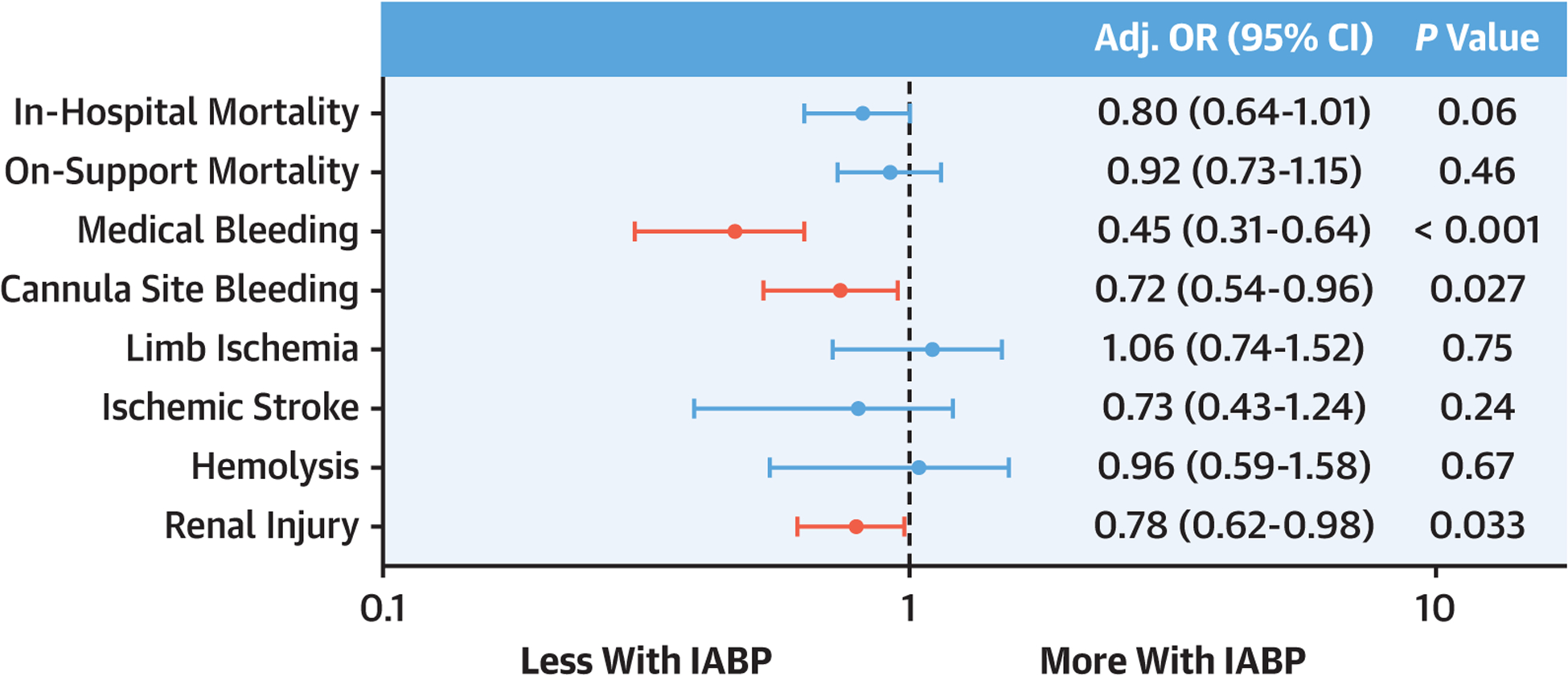
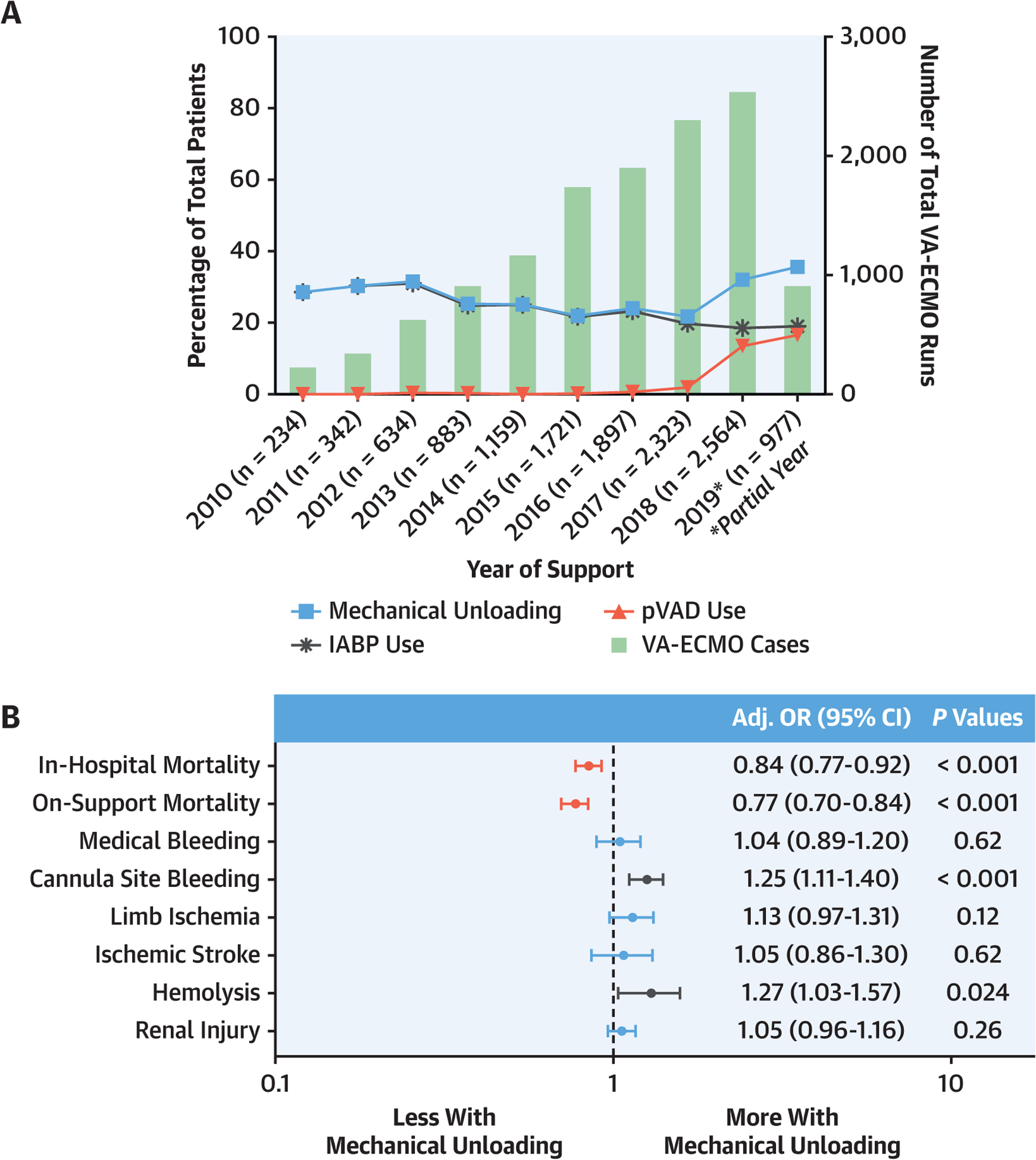
Results: Among 12,734 VA-ECMO patients, 3,399 (26.7%) received MU: 2,782 (82.9%) IABP and 580 (17.1%) pVAD. MU patients were older (age 56.3 vs 52.7 years) and, before extracorporeal membrane oxygenation, more often required >2 vasopressors (41.7% vs 27.2%) and had respiratory (21.1% vs 15.9%), renal (24.6% vs 15.8%), and liver failure (4.4% vs 3.1%) (all P < 0.001). MU patients had lower in-hospital mortality (56.6% vs 59.3%, P = 0.006), which persisted in multivariable modeling (adjusted OR [aOR]: 0.84; 95% CI: 0.77-0.92; P < 0.001). MU was associated with more cannula site bleeding (aOR: 1.25; 95% CI: 1.11-1.40; P < 0.001) and hemolysis (aOR: 1.27; 95% CI: 1.03-1.57; P = 0.02). Compared to pVAD, MU patients with IABP had similar mortality (aOR: 0.80; 95% CI: 0.64-1.01; P = 0.06) and less medical bleeding (aOR: 0.45; 95% CI: 0.31-0.64; P < 0.001), cannula site bleeding (aOR: 0.72; 95% CI: 0.54-0.96; P = 0.03), and renal injury (aOR: 0.78; 95% CI: 0.62-0.98; P = 0.03).
Conclusions: Among adults receiving VA-ECMO, MU was associated with lower in-hospital mortality despite increased complications including hemolysis and cannulation site bleeding. Compared to pVAD, MU with IABP was associated with similar mortality and lower complication rates.
Keywords: intra-aortic balloon pump; percutaneous ventricular assist device; survival; unloading; venoarterial extracorporeal membrane oxygenation.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Tonna has received a Career Development Award from the National Institutes of Health/National Heart, Lung, And Blood Institute (K23 HL141596); has received speaker fees and travel compensation from LivaNova, unrelated to this work; and is the Chair of the ELSO Registry Scientific Oversight Committee. Dr Kapur has received institutional research support and speaker/consulting honoraria from Abbott, Abiomed, Boston Scientific, Getinge, LivaNova, Medtronic, MDStart, Precardia, and Zoll. Dr Shaefi has received grants from the National Institutes of Health (K08 GM134220-01 and R01 DK125786-01). Dr Garan has received research support from Abbott Vascular and Verantos; and has received consultant fees from Abiomed and NupulseCV. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
ECMO: We Need to Vent About the Need to Vent!J Am Coll Cardiol. 2022 Apr 5;79(13):1251-1253. doi: 10.1016/j.jacc.2022.01.034. J Am Coll Cardiol. 2022. PMID: 35361347 No abstract available.
-
Who, When, and How to Vent During Venoarterial Extracorporeal Membrane Oxygenation?J Am Coll Cardiol. 2022 Nov 1;80(18):e149. doi: 10.1016/j.jacc.2022.04.072. J Am Coll Cardiol. 2022. PMID: 36302592 No abstract available.
-
Timing Matters.J Am Coll Cardiol. 2022 Nov 1;80(18):e151. doi: 10.1016/j.jacc.2022.04.069. J Am Coll Cardiol. 2022. PMID: 36302593 No abstract available.
-
Left Ventricular Venting Based on Acute Shock ECMO Phenotype.J Am Coll Cardiol. 2022 Nov 1;80(18):e153-e154. doi: 10.1016/j.jacc.2022.04.071. J Am Coll Cardiol. 2022. PMID: 36302594 Free PMC article. No abstract available.
-
Current Concepts of Mechanical Circulatory Support: Are We Ready to Unload?J Am Coll Cardiol. 2022 Nov 1;80(18):e155. doi: 10.1016/j.jacc.2022.04.070. J Am Coll Cardiol. 2022. PMID: 36302595 No abstract available.
-
Reply: Left Ventricular Mechanical Unloading During VA-ECMO: Not If, But Who and When?J Am Coll Cardiol. 2022 Nov 1;80(18):e157-e159. doi: 10.1016/j.jacc.2022.08.768. J Am Coll Cardiol. 2022. PMID: 36302596 No abstract available.
References
-
- Rao P, Khalpey Z, Smith R, Burkhoff D, Kociol RD. Venoarterial extracorporeal membrane oxygenation for cardiogenic shock and cardiac arrest. Circ Heart Fail. 2018;11:e004905. - PubMed
-
- Truby LK, Takeda K, Mauro C, et al. Incidence and implications of left ventricular distention during venoarterial extracorporeal membrane oxygenation support. ASAIO J. 2017;63:257–265. - PubMed
-
- Schrage B, Becher PM, Bernhardt A, et al. Left ventricular unloading is associated with lower mortality in cardiogenic shock patients treated with veno-arterial extracorporeal membrane oxygenation: results from an international, multicenter cohort study. Circulation. 2020;142(22): 2095–2106. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
