

Frailty, Guideline-Directed Medical Therapy, and Outcomes in HFrEF: From the GUIDE-IT Trial
- PMID: 35361446
- PMCID: PMC10539014
- DOI: 10.1016/j.jchf.2021.12.004
Frailty, Guideline-Directed Medical Therapy, and Outcomes in HFrEF: From the GUIDE-IT Trial
Abstract
Objectives: In this study, we sought to evaluate the association of frailty with the use of optimal guideline-directed medical therapy (GDMT) and outcomes in heart failure with reduced ejection fraction (HFrEF).
Background: The burden of frailty in HFrEF is high, and the patterns of GDMT use according to frailty status have not been studied previously.
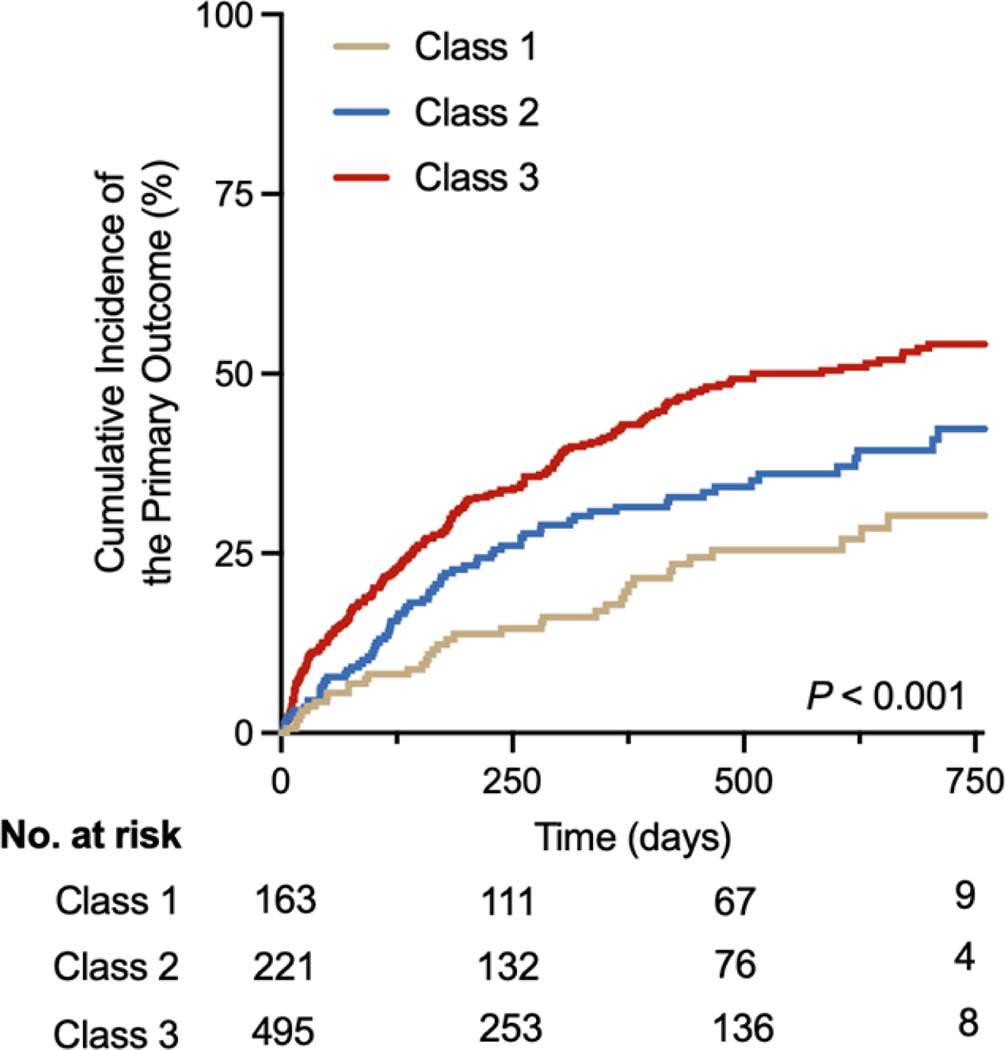
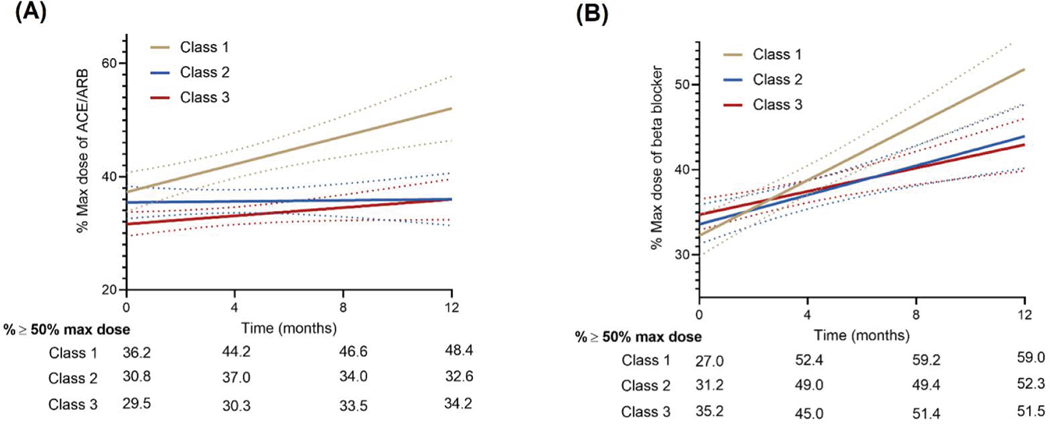
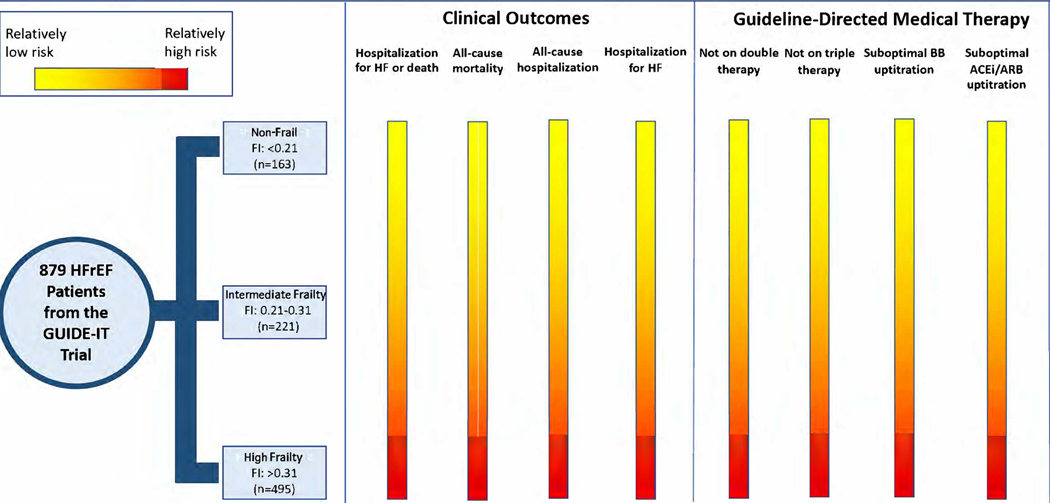
Methods: A post hoc analysis of patients with HFrEF enrolled in the GUIDE-IT (Guiding Evidence-Based Therapy Using Biomarker Intensified Treatment in Heart Failure) trial was conducted. Frailty was assessed with the use of a frailty index (FI) using a 38-variable deficit model, and participants were categorized into 3 groups: class 1: nonfrail, FI <0.21); class 2: intermediate frailty, FI 0.21-0.31), and class 3: high frailty, FI >0.31). Multivariate-adjusted Cox models were used to study the association of frailty status with clinical outcomes. Use of optimal GDMT over time (beta-blockers, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, and mineralocorticoid receptor antagonists) across frailty strata was assessed with the use of adjusted linear and logistic mixed-effect models.
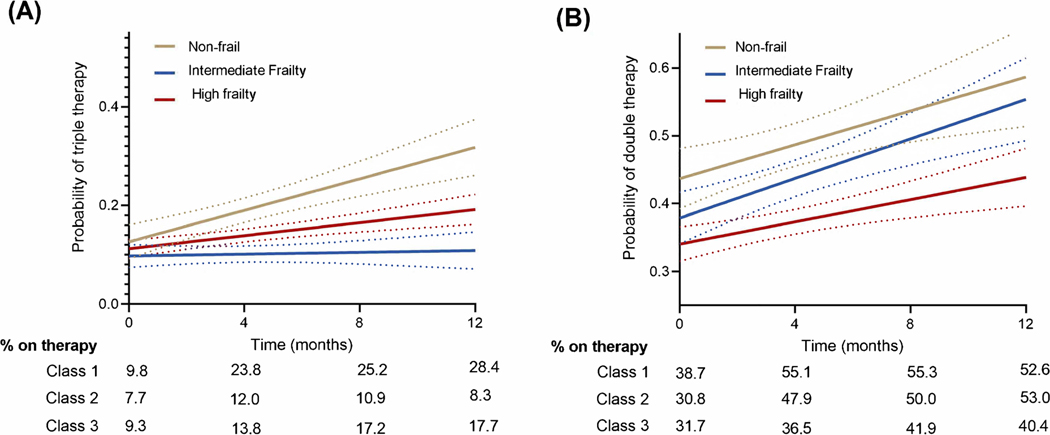
Results: The study included 879 participants, of which 56.3% had high frailty burden (class 3 FI). A higher frailty burden was associated with a significantly higher risk of HF hospitalization or death in adjusted Cox models: high frailty vs nonfrail HR: 1.76, 95% CI: 1.20-2.58. On follow-up, participants with high frailty burden also had a significantly lower likelihood of achieving optimal GDMT: high frailty vs non-frail GDMT triple therapy use at study end: 17.7% vs 28.4%; P interaction, frailty class × time <0.001.
Conclusions: Patients with HFrEF with a high burden of frailty have a significantly higher risk for adverse clinical outcomes and are less likely to be initiated and up-titrated on an optimal GDMT regimen.
Keywords: frailty; guideline-directed medical therapy; heart failure with reduced ejection fraction; mortality.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The GUIDE-IT study was funded by grants HL105448, HL105451, and HL105457 from the National Institutes of Health, and Roche Diagnostics provided support for NT-proBNP testing. Dr Greene has received research support from the Duke University Department of Medicine Chair’s Research Award, American Heart Association, Amgen, AstraZeneca, Bristol Myers Squibb, Cytokinetics, Merck, Novartis, Pfizer, and Sanofi; has served on advisory boards for Amgen, AstraZeneca, Bristol Myers Squibb, Cytokinetics, and Sanofi; and serves as a consultant for Amgen, Bayer, Bristol Myers Squibb, Merck, and Vifor. Dr Fonarow is a consultant for Abbott, Amgen, AstraZeneca, Bayer, Janssen, Medtronic, Merck, and Novartis, and Associate Section Editor for the JAMA Cardiology. Dr Anker has received research support from Vifor International and Abbott Vascular; and fees for consultancy and/or speaking from AstraZeneca, Bayer, Boehringer Ingelheim, Respicardia, Impulse Dynamics, Janssen, Novartis, Servier, and Vifor International. Dr Felker has received research grants from the National Heart, Lung, and Blood Institute, American Heart Association, Amgen, Bayer Merck, Cytokinetics, Myokardia; has acted as a consultant to Novartis, Amgen, Bristol Myers Squibb, Cytokinetics, Medtronic, Cardionomic, Boehringer-Ingelheim, American Regent, Abbott, AstraZeneca, Reprieve, and Sequana; and has served on clinical end point committees/data safety monitoring boards for Amgen, Merck, Medtronic, EBR Systems, V-Wave, LivaNova, Siemens, and Rocket Pharma. Dr Januzzi has received grant support from Roche Diagnostics, Abbott Diagnostics, Singulex, Prevencio, Novartis, and Cleveland Heart Labs; has received consulting income from Roche Diagnostics, Abbott, Prevencio, and Critical Diagnostics; and participates in clinical end point committees/data safety monitoring boards for Siemens Diagnostics, Novartis, Bayer, AbbVie, and Amgen. Dr Butler has acted as a consultant to Abbott, Adrenomed, Amgen, Applied Therapeutics, Array, AstraZeneca, Bayer, Boehringer Ingelheim, CVRx, G3 Pharma, Impulse Dynamics, Innolife, Janssen, LivaNova, Luitpold, Medtronic, Merck, Novartis, NovoNordisk, Relypsa, Sequana Medical, V-Wave Limited, and Vifor; and has served on speaker bureaus for Novartis, Boehringer Ingelheim–Lilly, AstraZeneca, and Janssen. Dr Pandey is supported by the Texas Health Resources Clinical Scholars Program; and has served on the advisory board of Roche Diagnostics. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
"Don't Be Frail to Optimize Heart Failure Therapies!".JACC Heart Fail. 2022 Apr;10(4):276-277. doi: 10.1016/j.jchf.2022.01.006. Epub 2022 Mar 9. JACC Heart Fail. 2022. PMID: 35361447 No abstract available.
References
-
- Greene SJ, Butler J, Albert NM et al. Medical Therapy for Heart Failure With Reduced Ejection Fraction: The CHAMP-HF Registry. J Am Coll Cardiol 2018;72:351–366. - PubMed
-
- Fried LP, Tangen CM, Walston J et al. Frailty in Older Adults: Evidence for a Phenotype. The Journals of Gerontology: Series A 2001;56:M146–M157. - PubMed
-
- Rockwood K, Mitnitski A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin Geriatr Med 2011;27:17–26. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
