

Angiographically Occult Subarachnoid Hemorrhage: Yield of Repeat Angiography, Influence of Initial CT Bleed Pattern, and Sources of Diagnostic Error in 242 Consecutive Patients
- PMID: 35361576
- PMCID: PMC9089267
- DOI: 10.3174/ajnr.A7483
Angiographically Occult Subarachnoid Hemorrhage: Yield of Repeat Angiography, Influence of Initial CT Bleed Pattern, and Sources of Diagnostic Error in 242 Consecutive Patients
Abstract
Background and purpose: Nearly 20% of patients with spontaneous SAH have no definitive source on initial DSA. The purpose of this study was to investigate the timing and yield of repeat DSA, to clarify the influence of initial CT bleed pattern, and to characterize sources of diagnostic error in this scenario.
Materials and methods: We evaluated the yield of repeat DSA and clinical outcomes stratified by hemorrhage pattern on CT in consecutive patients with nontraumatic SAH with negative initial DSA findings at a referral center. Cases in which the culprit lesion was subsequently diagnosed were classified as physiologically occult (ie, undetectable) on the initial DSA, despite adequate technique and interpretation or misdiagnosed due to operator-dependent error.
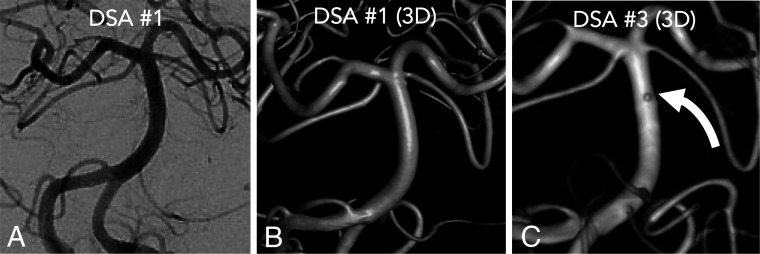
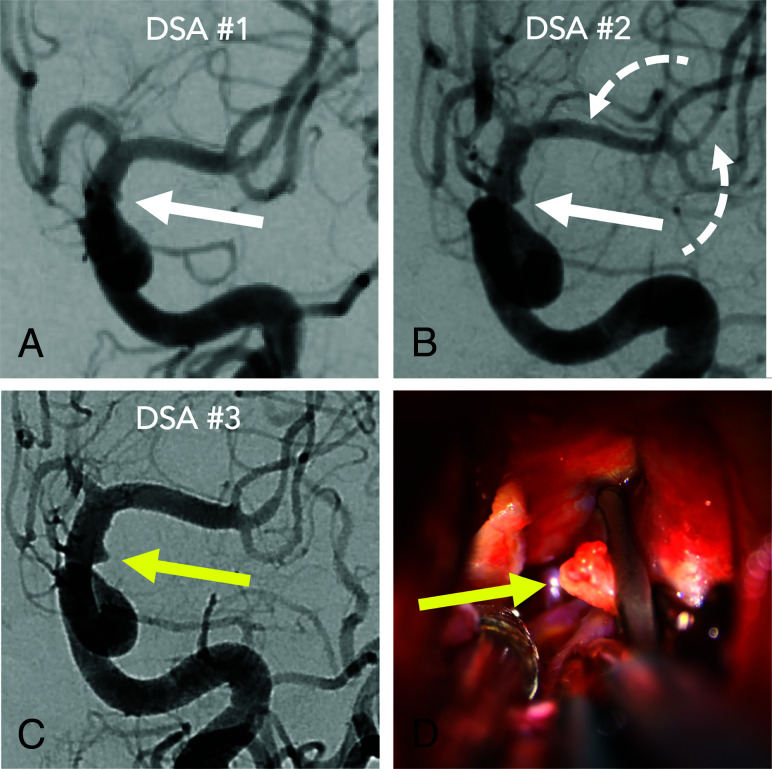
Results: Two hundred forty-two of 1163 (20.8%) patients with spontaneous SAH had negative initial DSA findings between 2009 and 2018. The SAH CT pattern was nonperimesencephalic (41%), perimesencephalic (36%), sulcal (18%), and CT-negative (5%). Repeat DSA in 135/242 patients (55.8%) revealed a source in 10 patients (7.4%): 4 saccular aneurysms, 4 atypical aneurysms, and 2 arteriovenous shunts. The overall yield of repeat DSA was 11.3% with nonperimesencephalic and 2.2% for perimesencephalic patterns. The yield of the second and third DSAs with a nonperimesencephalic pattern was 7.7% and 12%, respectively. Physiologically occult lesions accounted for 6/242 (2.5%) and operator-dependent errors accounted for 7/242 (2.9%) of all angiographically occult lesions on the first DSA.
Conclusions: Atypical aneurysms and small arteriovenous shunts are important causes of SAH negative on angiography. Improving DSAs technique can modestly reduce the need for repeat DSA; however, a small fraction of SAH sources remain occult despite adequate technique. These findings support the practice of repeating DSA in patients with a nonperimesencephalic SAH pattern.
© 2022 by American Journal of Neuroradiology.
Figures
References
-
- Dalyai R, Chalouhi N, Theofanis T, et al. . Subarachnoid hemorrhage with negative initial catheter angiography: a review of 254 cases evaluating patient clinical outcome and efficacy of short- and long-term repeat angiography. Neurosurgery 2013;72:646–52; discussion 651–52 10.1227/NEU.0b013e3182846de8 - DOI - PubMed