

Intravenous methylprednisolone pulses in hospitalised patients with severe COVID-19 pneumonia: a double-blind, randomised, placebo-controlled trial
- PMID: 35361632
- PMCID: PMC8971731
- DOI: 10.1183/13993003.00025-2022
Intravenous methylprednisolone pulses in hospitalised patients with severe COVID-19 pneumonia: a double-blind, randomised, placebo-controlled trial
Abstract
Rationale: Pulse glucocorticoid therapy is used in hyperinflammation related to coronavirus disease 2019 (COVID-19). We evaluated the efficacy and safety of pulse intravenous methylprednisolone in addition to standard treatment in COVID-19 pneumonia.
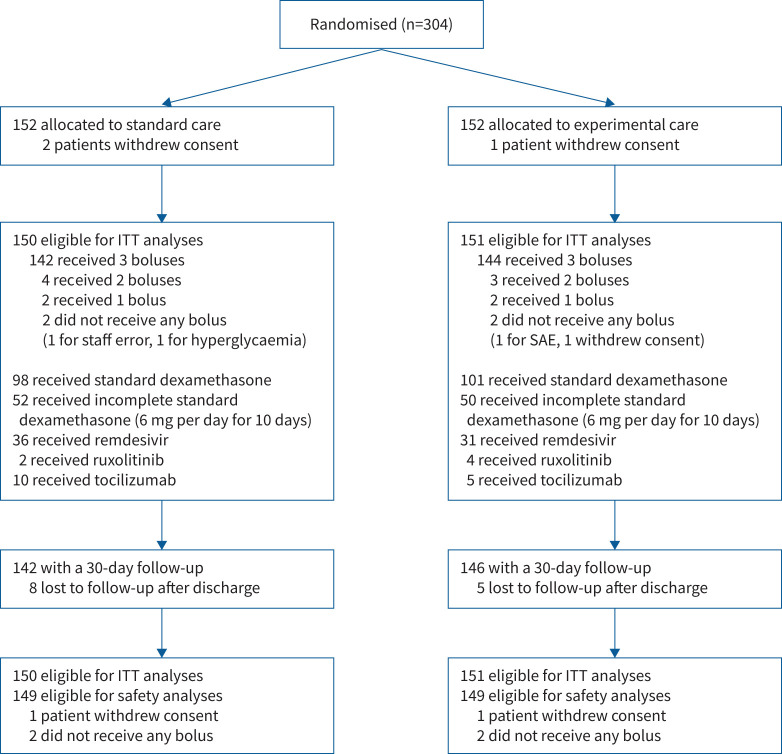
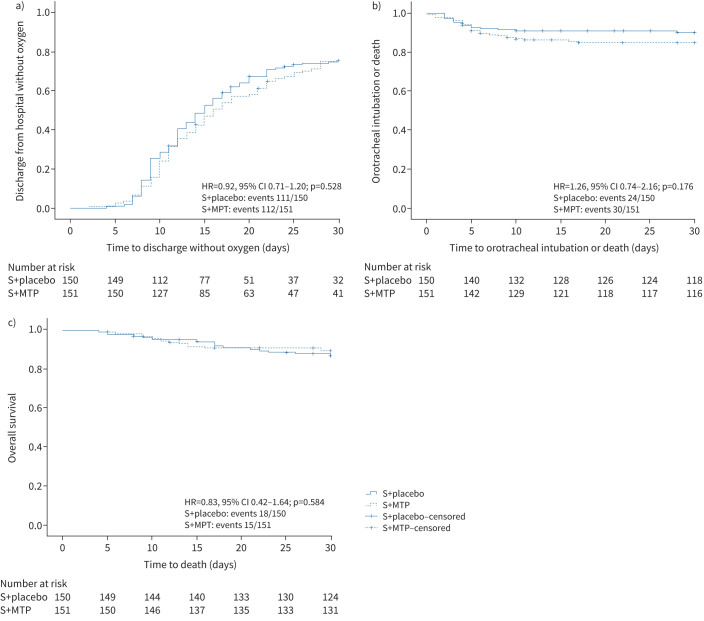
Methods: In this multicentre, randomised, double-blind, placebo-controlled trial, 304 hospitalised patients with COVID-19 pneumonia were randomised to receive 1 g of methylprednisolone intravenously for three consecutive days or placebo in addition to standard dexamethasone. The primary outcome was the duration of patient hospitalisation, calculated as the time interval between randomisation and hospital discharge without the need for supplementary oxygen. The key secondary outcomes were survival free from invasive ventilation with orotracheal intubation and overall survival.
Results: Overall, 112 (75.4%) out of 151 patients in the pulse methylprednisolone arm and 111 (75.2%) of 150 in the placebo arm were discharged from hospital without oxygen within 30 days from randomisation. Median time to discharge was similar in both groups (15 days, 95% CI 13.0-17.0 days and 16 days, 95% CI 13.8-18.2 days, respectively; hazard ratio (HR) 0.92, 95% CI 0.71-1.20; p=0.528). No significant differences between pulse methylprednisolone and placebo arms were observed in terms of admission to intensive care unit with orotracheal intubation or death (20.0% versus 16.1%; HR 1.26, 95% CI 0.74-2.16; p=0.176) or overall mortality (10.0% versus 12.2%; HR 0.83, 95% CI 0.42-1.64; p=0.584). Serious adverse events occurred with similar frequency in the two groups.
Conclusions: Methylprenisolone pulse therapy added to dexamethasone was not of benefit in patients with COVID-19 pneumonia.
Trial registration: ClinicalTrials.gov NCT04673162.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: The authors declare no competing interests.
Figures
Comment in
-
Are intravenous corticosteroid pulses superior to low dose corticosteroids in patients with severe COVID-19?Eur Respir J. 2022 Oct 20;60(4):2201220. doi: 10.1183/13993003.01220-2022. Print 2022 Oct. Eur Respir J. 2022. PMID: 35777764 Free PMC article.
References
-
- Cassone G, Dolci G, Besutti G, et al. Acute-phase reactants during tocilizumab therapy for severe COVID-19 pneumonia. Clin Exp Rheumatol 2020; 38: 1215–1222. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical