

Asthma remission: what is it and how can it be achieved?
- PMID: 35361633
- PMCID: PMC9630609
- DOI: 10.1183/13993003.02583-2021
Asthma remission: what is it and how can it be achieved?
Abstract
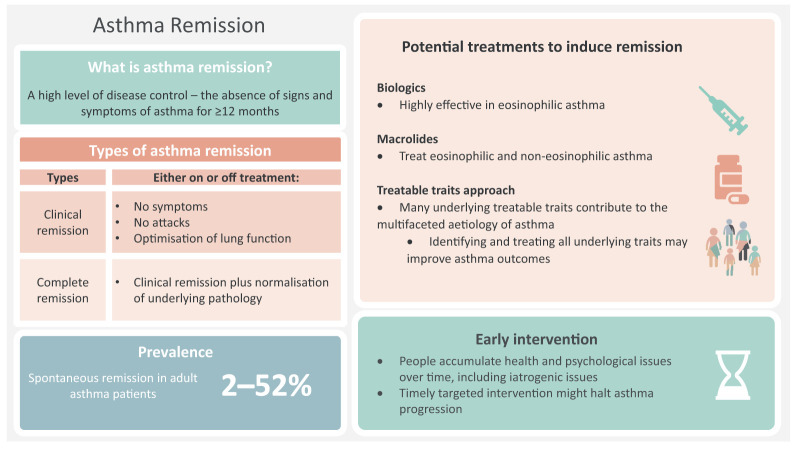
Asthma treatment goals currently focus on symptom and exacerbation control rather than remission. Remission is not identical to cure, but is a step closer. This review considers the current definitions of remission in asthma, the prevalence and predictors, the pathophysiology of remission, the possibility of achieving it using the available treatment options, and the future research directions. Asthma remission is characterised by a high level of disease control, including the absence of symptoms and exacerbations, and normalisation or optimisation of lung function with or without ongoing treatment. Even in those who develop a symptomatic remission of asthma, persistent pathological abnormalities are common, leading to a risk of subsequent relapse at any time. Complete remission requires normalisation or stabilisation of any underlying pathology in addition to symptomatic remission. Remission is possible as part of the natural history of asthma, and the prevalence of remission in the adult asthma population varies between 2% and 52%. The factors associated with remission include mild asthma, better lung function, better asthma control, younger age, early-onset asthma, shorter duration of asthma, milder bronchial hyperresponsiveness, fewer comorbidities and smoking cessation or never smoking. Although previous studies have not targeted treatment-induced remission, there is some evidence to show that the current long-term add-on therapies such as biologics and azithromycin can achieve some criteria for asthma remission on treatment, at least in a subgroup of patients. However, more research is required. Long-term remission could be included as a therapeutic goal in studies of asthma treatments.
Copyright ©The authors 2022.
Conflict of interest statement
Number 7 in the series “Innovations in asthma and its treatment” Edited by P. O'Byrne and I. Pavord Conflict of interest: D. Thomas has nothing to disclose. V.M. McDonald reports grants and personal fees from GSK and AstraZeneca, and personal fees from Menarini, outside the submitted work. I.D. Pavord reports speaker's honoraria for sponsored meetings from AstraZeneca, Boehringer Ingelheim, Aerocrine, Almirall, Novartis, Teva, Chiesi, Sanofi, Regeneron and GSK; payments for organising educational events from AstraZeneca, GSK, Sanofi, Regeneron and Teva; honoraria for attending advisory panels with Genentech, Sanofi, Regeneron, AstraZeneca, Boehringer Ingelheim, GSK, Novartis, Teva, Merck, Circassia, Chiesi, Knopp, Almirall, Dey Pharma, Napp Pharmaceuticals, RespiVert and Schering-Plough; sponsorship to attend international scientific meetings from Boehringer Ingelheim, GSK, AstraZeneca, Teva, Sanofi, Regeneron and Chiesi; grants from Chiesi to support a Phase II clinical trial in Oxford; and is co-patent holder of the rights to the Leicester Cough Questionnaire and has received payments for its use in clinical trials from Merck, Bayer and Insmed. P.G. Gibson reports grants and personal fees from GSK and AstraZeneca, and personal fees from Novartis, Chiesi and Sanofi, outside the submitted work.
Figures
References
-
- Global Asthma Network . The Global Asthma Report 2018. 2018. http://globalasthmareport.org/resources/Global_Asthma_Report_2018.pdf Date last accessed: 26 March 2022.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical