

Effect of neoadjuvant chemotherapy on the immune microenvironment in gastric cancer as determined by multiplex immunofluorescence and T cell receptor repertoire analysis
- PMID: 35361730
- PMCID: PMC8971786
- DOI: 10.1136/jitc-2021-003984
Effect of neoadjuvant chemotherapy on the immune microenvironment in gastric cancer as determined by multiplex immunofluorescence and T cell receptor repertoire analysis
Abstract
Background: The combination of immune checkpoint blockade and chemotherapy has revolutionized the treatment of advanced gastric cancer (GC). It is crucial to unravel chemotherapy-induced tumor microenvironment (TME) modulation and identify which immunotherapy would improve antitumor effect.
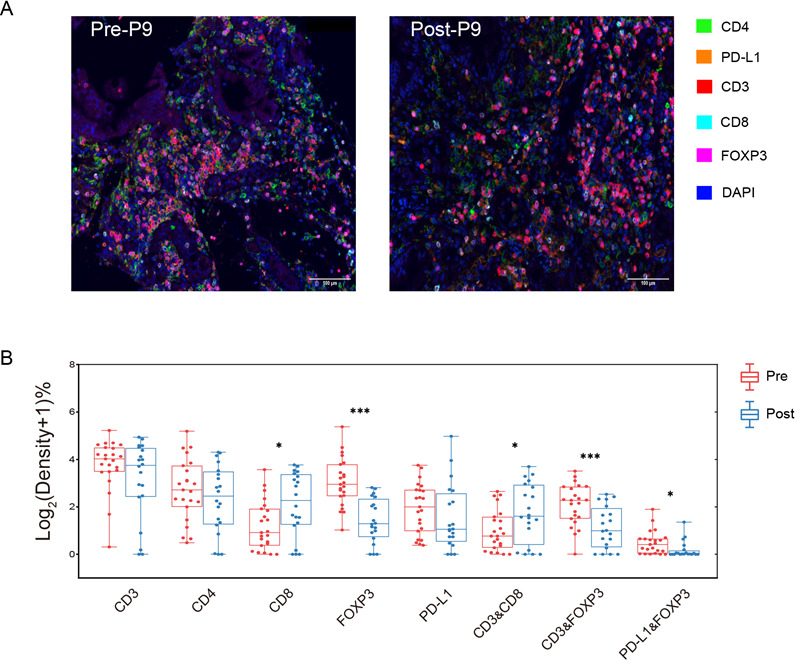
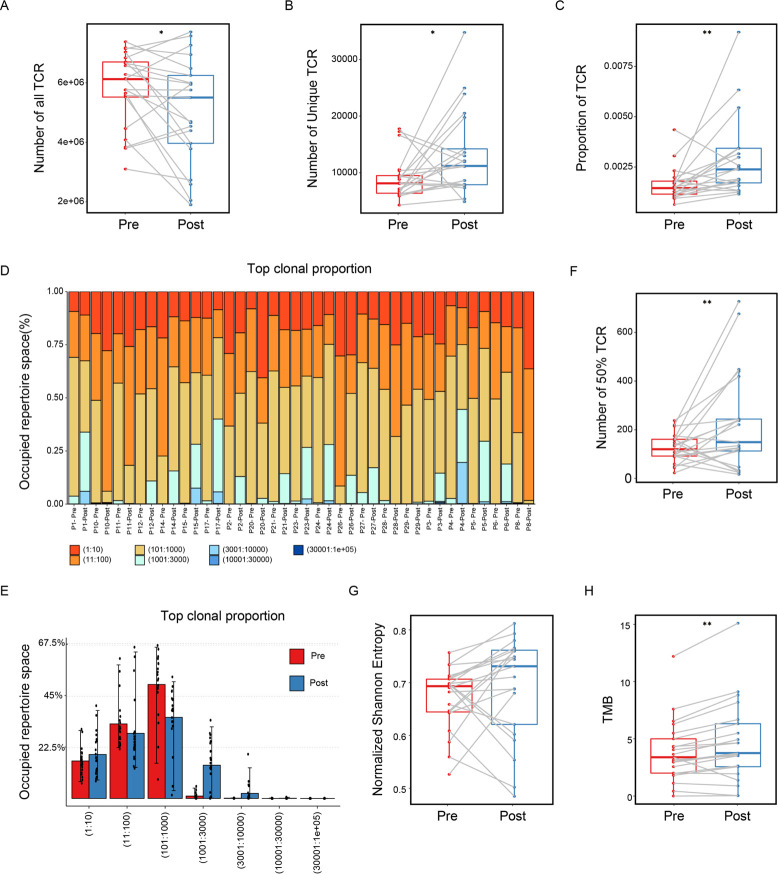
Methods: In this study, tumor-associated immune cells (TAICs) infiltration in residual tumor after neoadjuvant chemotherapy (NAC) together with 1075 cases of treatment-naïve GC patients was analyzed first. Then we performed multiplex fluorescence staining of a panel of immune markers (CD3, CD4, CD8, FOXP3 and PDL1) and T cell receptor β-chain sequencing to phenotype and enumerate T cell subpopulations and clonal expansion in paired GC samples (prechemotherapy and postchemotherapy) from another cohort of 30 cases of stage II/III GC patients.
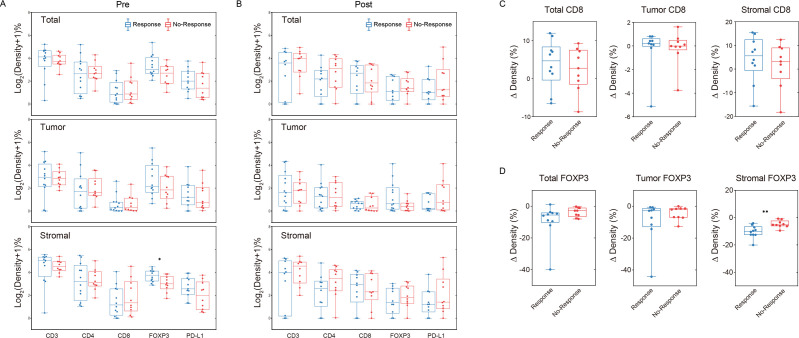
Results: Infiltration of CD68+ macrophages in residual tumors after NAC was significantly decreased compared with treatment-naïve GC patients, while no significant difference observed with respect to other immune markers. In residual tumors, post-NAC CD8 +T cells and CD68+ macrophages levels were significantly associated with chemotherapy response. Post-NAC CD8+ T cell levels remained as an independent predictor for favorable prognosis. Furthermore, when comparing the paired samples before and after NAC from 30 cases of stage II/III GC patients, we found FOXP3+ regulatory T cells proportion significantly decreased after chemotherapy. Pre-NAC FOXP3+ T reg cells level was much richer in the response group and decreased more significantly in the stromal compartment. CD8+ cytotoxic T lymphocytes levels were elevated after chemotherapy, which was more significant in the group treated with XELOX regimen and in patients with better response, consistent with the TCR diversity elevation.
Conclusions: These findings have deepened our understanding of the immune modulating effect of chemotherapy and suggest that the immune profile of specimens after standard chemotherapy should be considered for the personalized immunotherapy to ultimately improve clinical outcome in patients with GC.
Keywords: gastrointestinal neoplasms; tumor biomarkers; tumor microenvironment.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


References
-
- Hindson J. Nivolumab plus chemotherapy for advanced gastric cancer and oesophageal adenocarcinoma. Nat Rev Gastroenterol Hepatol 2021. - PubMed
-
- Moehler M, Shitara K, Garrido M, et al. LBA6_PR Nivolumab (nivo) plus chemotherapy (chemo) versus chemo as first-line (1L) treatment for advanced gastric cancer/gastroesophageal junction cancer (GC/GEJC)/esophageal adenocarcinoma (EAC): First results of the CheckMate 649 study. Ann Oncol 2020;31:S1191. 10.1016/j.annonc.2020.08.2296 - DOI
-
- Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet 2021;398:27–40. 10.1016/S0140-6736(21)00797-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous