

Targeted Metagenomic Sequencing-based Approach Applied to 2146 Tissue and Body Fluid Samples in Routine Clinical Practice
- PMID: 35362534
- PMCID: PMC9662179
- DOI: 10.1093/cid/ciac247
Targeted Metagenomic Sequencing-based Approach Applied to 2146 Tissue and Body Fluid Samples in Routine Clinical Practice
Abstract
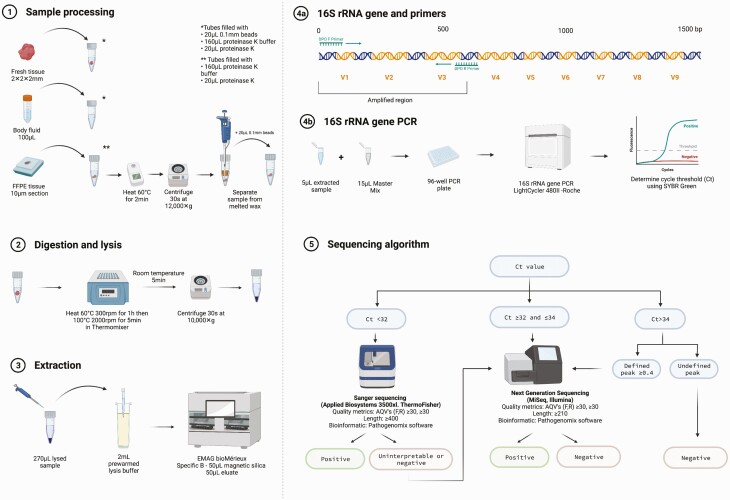
Background: The yield of next-generation sequencing (NGS) added to a Sanger sequencing-based 16S ribosomal RNA (rRNA) gene polymerase chain reaction (PCR) assay was evaluated in clinical practice for diagnosis of bacterial infection.
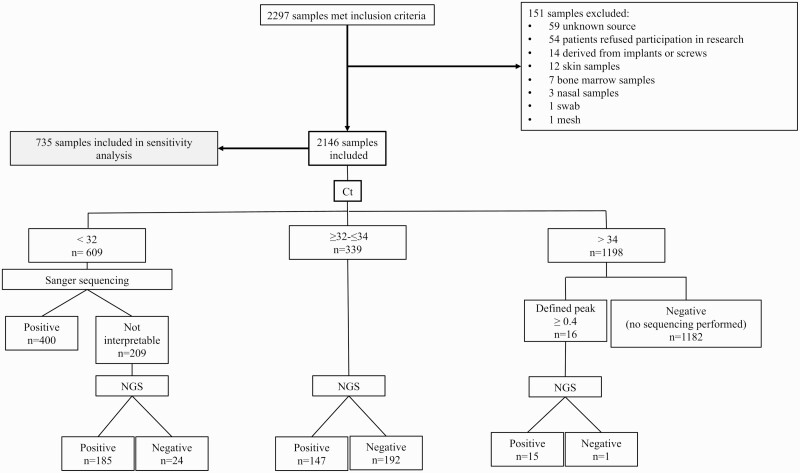
Methods: PCR targeting the V1 to V3 regions of the 16S rRNA gene was performed, with amplified DNA submitted to Sanger sequencing and/or NGS (Illumina MiSeq) or reported as negative, depending on the cycle threshold value. A total of 2146 normally sterile tissues or body fluids were tested between August 2020 and March 2021. Clinical sensitivity was assessed in 579 patients from whom clinical data were available.
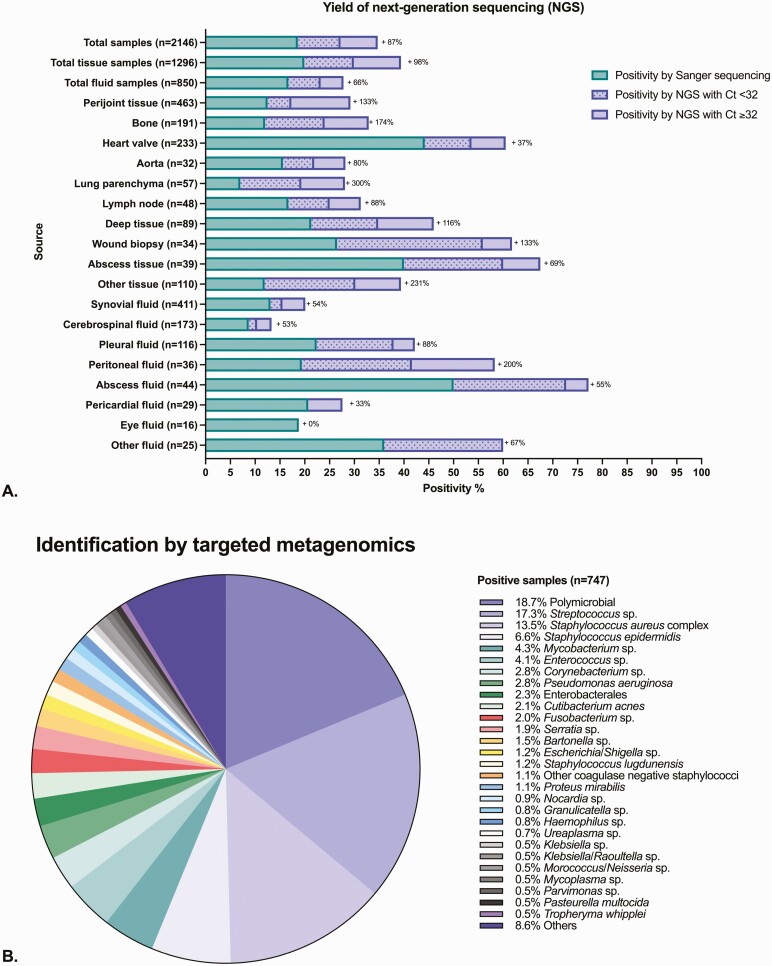
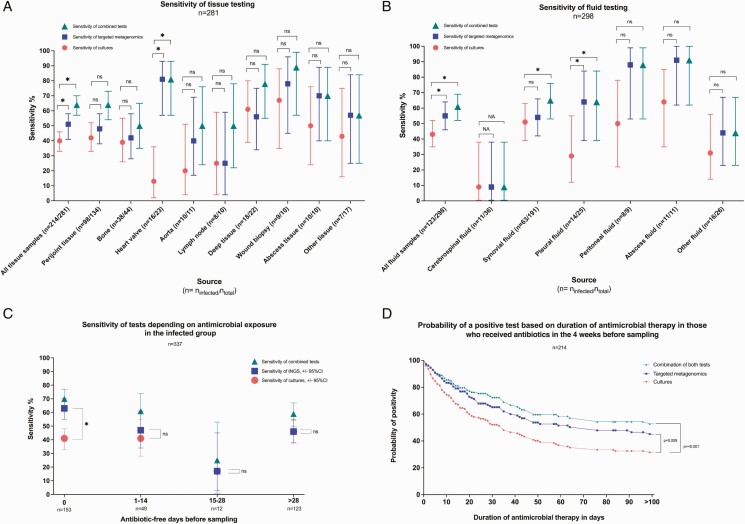
Results: Compared with Sanger sequencing alone (400 positive tests), positivity increased by 87% by adding NGS (347 added positive tests). Clinical sensitivity of the assay that incorporated NGS was 53%, which was higher than culture (42%, P < .001), with an impact on clinical decision-making in 14% of infected cases. Clinical sensitivity in the subgroup that received antibiotics at sampling was 41% for culture and 63% for the sequencing assay (P < .001).
Conclusions: Adding NGS to Sanger sequencing of the PCR-amplified 16S rRNA gene substantially improved test positivity. In the patient population studied, the assay was more sensitive than culture, especially in patients who had received antibiotic therapy.
Keywords: 16S ribosomal RNA gene PCR; clinical metagenomics; targeted metagenomics; tissue and body fluids.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. R.P. reports grants from ContraFect, TenNor Therapeutics Limited, and BioFire; is a consultant to Curetis, Specific Technologies, Next Gen Diagnostics, PathoQuest, Selux Diagnostics, 1928 Diagnostics, PhAST, Torus Biosystems, Day Zero Diagnostics, Mammoth Biosciences, and Qvella; monies are paid to Mayo Clinic. Mayo Clinic and R.P. have relationships with Adaptive Phage Therapeutics and Pathogenomix. R.P. is a consultant to Netflix and CARB-X; has a patent on Bordetella pertussis/parapertussis polymerase chain reaction issued, a patent on a device/method for sonication with royalties paid by Samsung to Mayo Clinic, and a patent on an antibiofilm substance issued; receives honoraria from the National Board of Medical Examiners, Up-to-Date, and the Infectious Diseases Board Review Course; reports being Chair, ASM Governance Committee and Member, Finance Committee (ASM); and reports an editor’s stipend from the Infectious Diseases Society of America. N.W. reports royalties or licenses from Roche Diagnostics; and a leadership or fiduciary role for Clinical and Laboratory Standards Institute working groups and document development committees. All authors are employees of Mayo Clinic. M.W. reports having a relationship with Pathogenomix through Mayo Clinic. All remaining authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Lefterova MI, Suarez CJ, Banaei N, Pinsky BA.. Next-generation sequencing for infectious disease diagnosis and management: a report of the Association for Molecular Pathology. J Mol Diagn 2015; 17:623–34. - PubMed
-
- Fournier PE, Thuny F, Richet H, et al. Comprehensive diagnostic strategy for blood culture-negative endocarditis: a prospective study of 819 new cases. Clin Infect Dis 2010; 51:131–40. - PubMed
-
- Harbarth S, Nobre V, Pittet D.. Does antibiotic selection impact patient outcome?. Clin Infect Dis 2007; 44:87–93. - PubMed
-
- Spyridakis E, Gerber JS, Schriver E, et al. Clinical features and outcomes of children with culture-negative septic arthritis. J Pediatric Infect Dis Soc 2019; 8:228–34. - PubMed
