

Precision Medicine in Pancreatic Cancer: Patient-Derived Organoid Pharmacotyping Is a Predictive Biomarker of Clinical Treatment Response
- PMID: 35363262
- PMCID: PMC9357072
- DOI: 10.1158/1078-0432.CCR-21-4165
Precision Medicine in Pancreatic Cancer: Patient-Derived Organoid Pharmacotyping Is a Predictive Biomarker of Clinical Treatment Response
Abstract
Purpose: Patient-derived organoids (PDO) are a promising technology to support precision medicine initiatives for patients with pancreatic ductal adenocarcinoma (PDAC). PDOs may improve clinical next-generation sequencing (NGS) and enable rapid ex vivo chemotherapeutic screening (pharmacotyping).
Experimental design: PDOs were derived from tissues obtained during surgical resection and endoscopic biopsies and studied with NGS and pharmacotyping. PDO-specific pharmacotype is assessed prospectively as a predictive biomarker of clinical therapeutic response by leveraging data from a randomized controlled clinical trial.
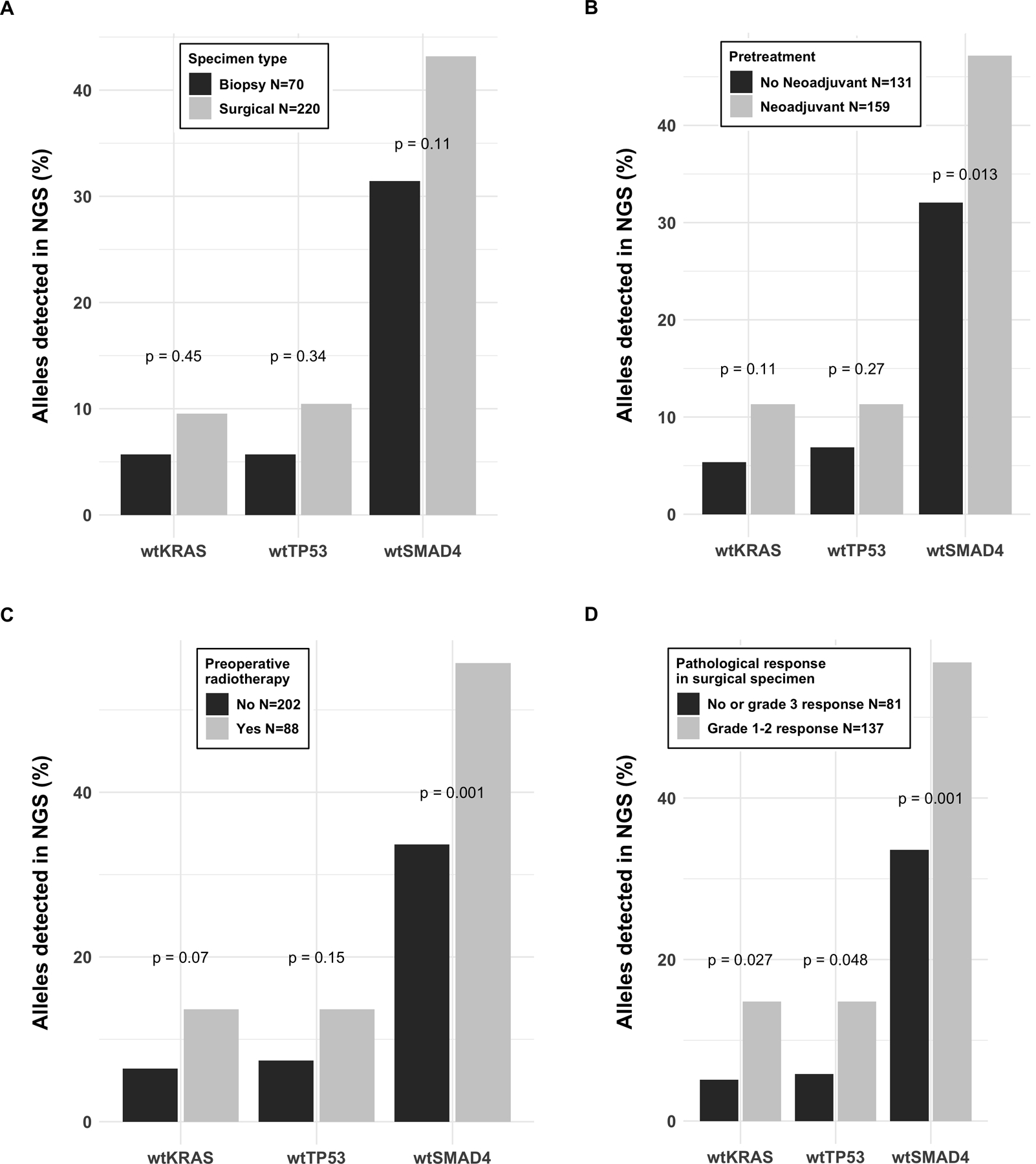
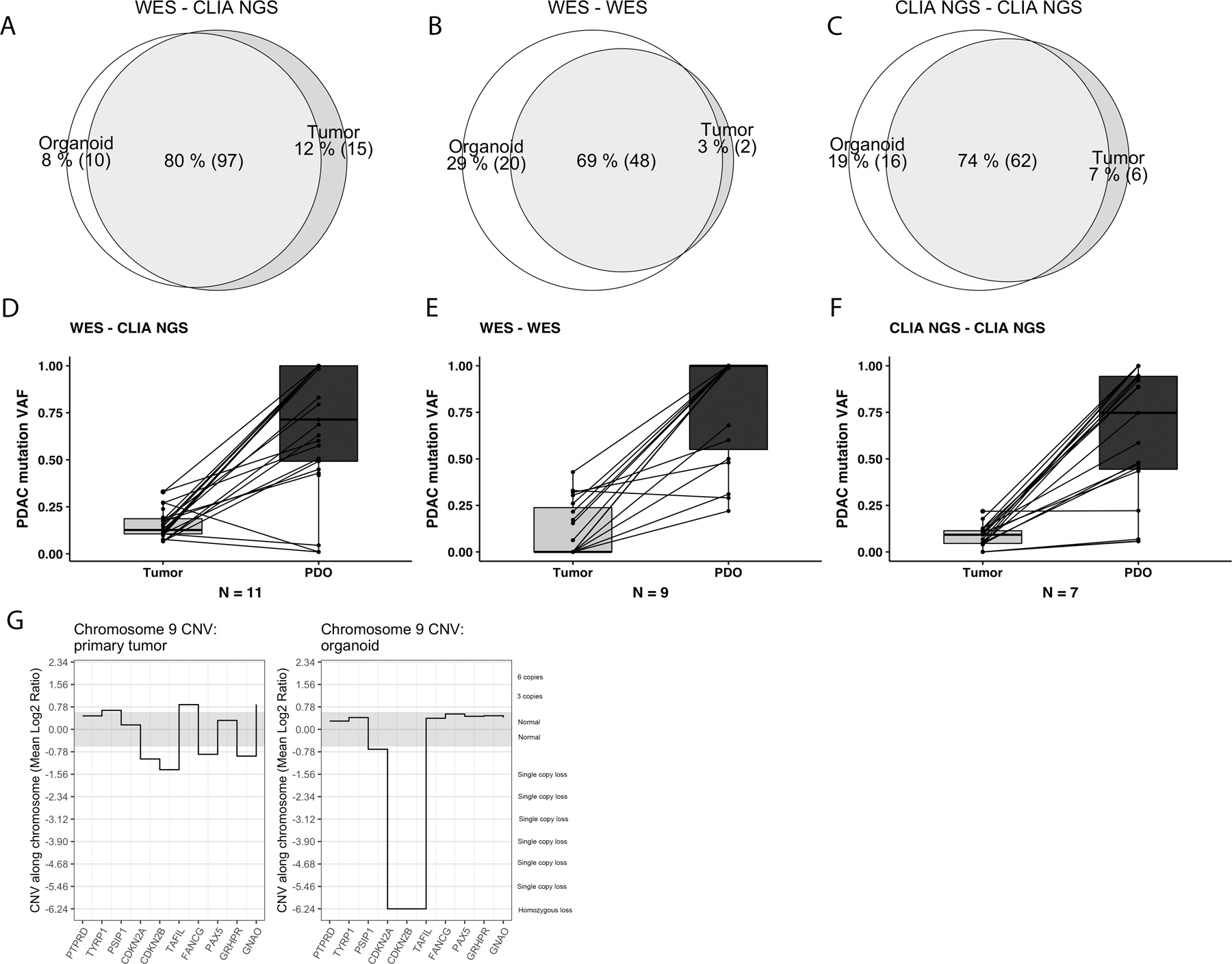
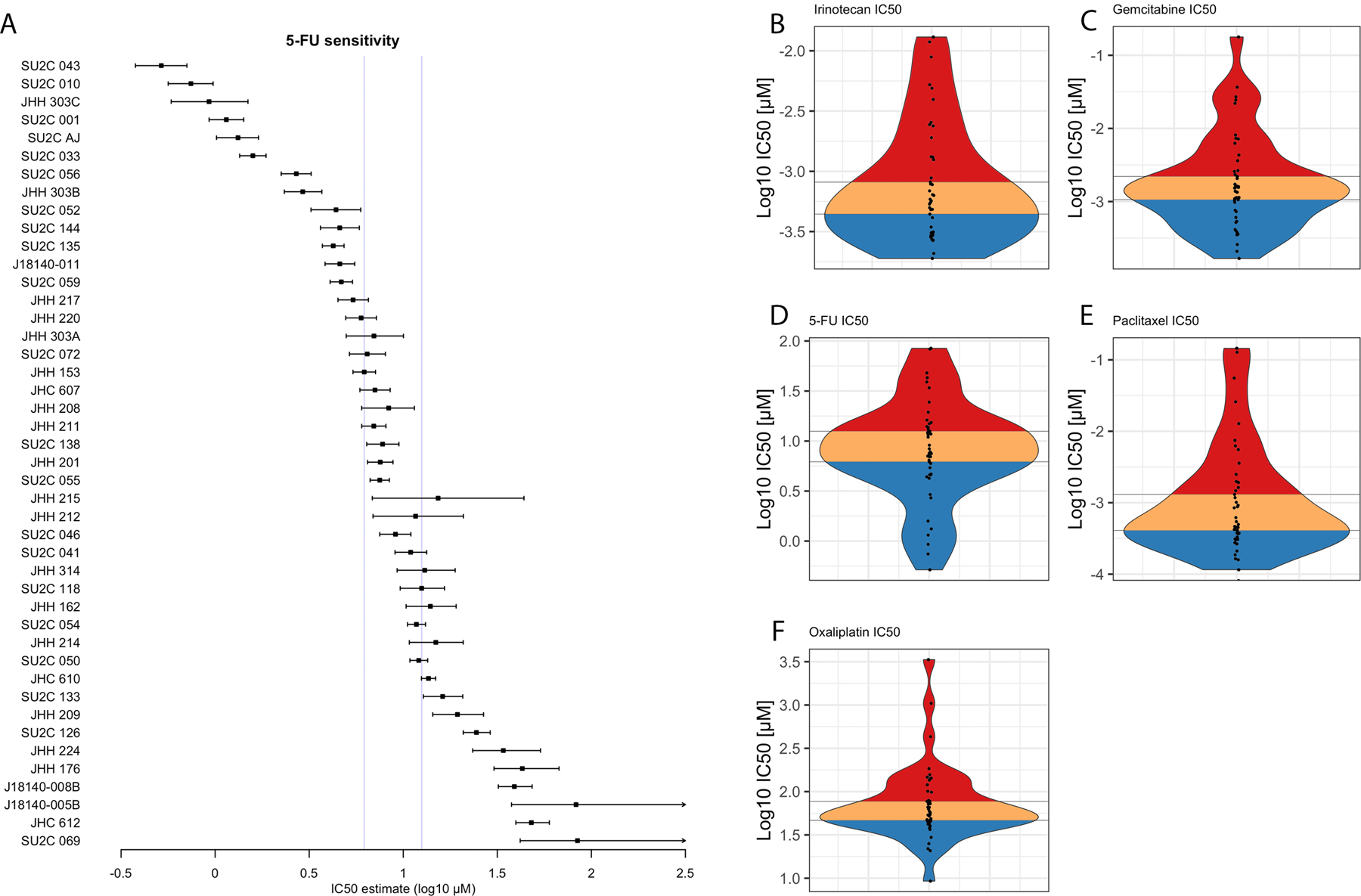
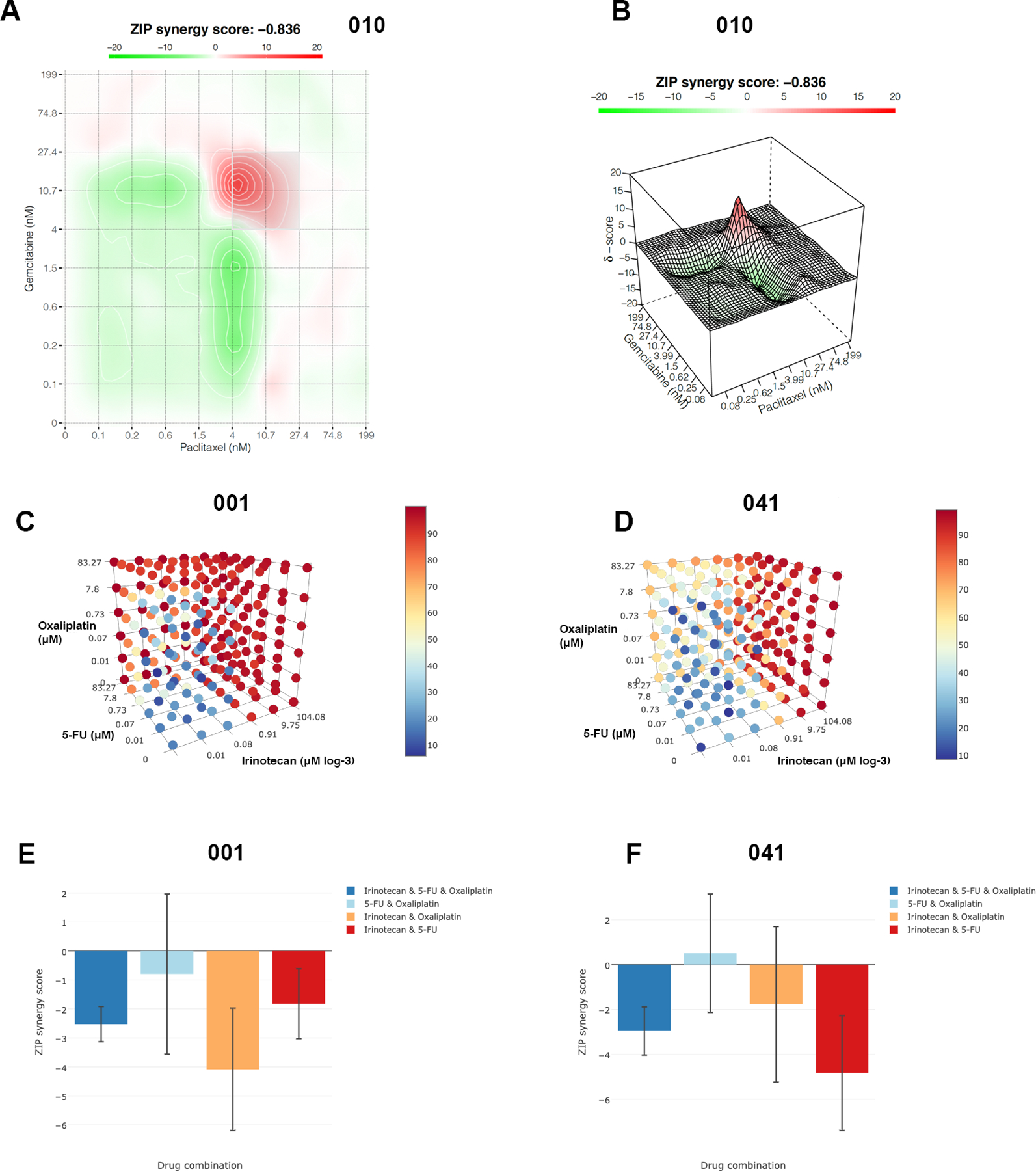
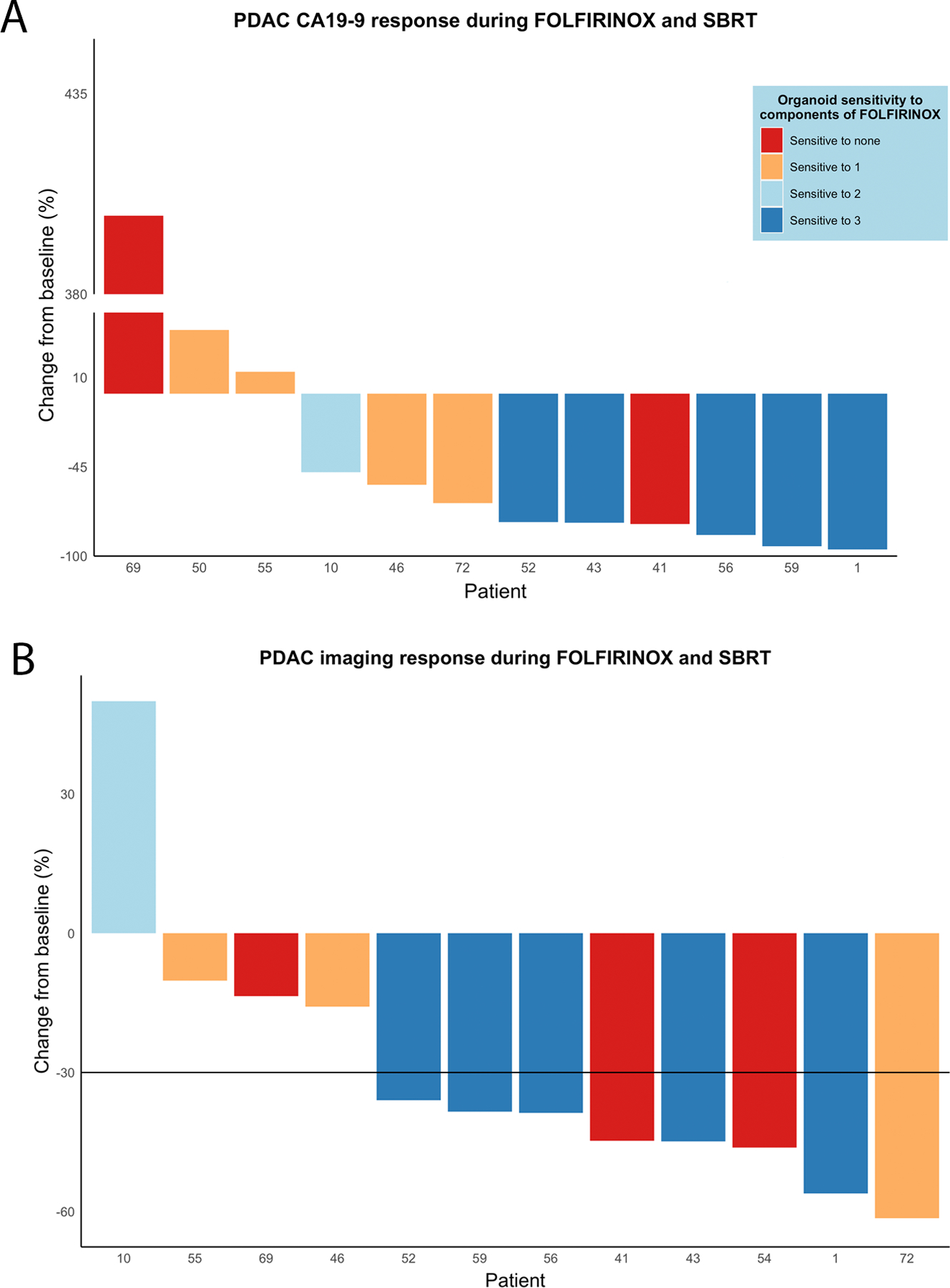
Results: Clinical sequencing pipelines often fail to detect PDAC-associated somatic mutations in surgical specimens that demonstrate a good pathologic response to previously administered chemotherapy. Sequencing the PDOs derived from these surgical specimens, after biomass expansion, improves the detection of somatic mutations and enables quantification of copy number variants. The detection of clinically relevant mutations and structural variants is improved following PDO biomass expansion. On clinical trial, PDOs were derived from biopsies of treatment-naïve patients prior to treatment with FOLFIRINOX (FFX). Ex vivo PDO pharmacotyping with FFX components predicted clinical therapeutic response in these patients with borderline resectable or locally advanced PDAC treated in a neoadjuvant or induction paradigm. PDO pharmacotypes suggesting sensitivity to FFX components were associated with longitudinal declines of tumor marker, carbohydrate-antigen 19-9 (CA-19-9), and favorable RECIST imaging response.
Conclusions: PDOs established from tissues obtained from patients previously receiving cytotoxic chemotherapies can be accomplished in a clinically certified laboratory. Sequencing PDOs following biomass expansion improves clinical sequencing quality. High in vitro sensitivity to standard-of-care chemotherapeutics predicts good clinical response to systemic chemotherapy in PDAC. See related commentary by Zhang et al., p. 3176.
©2022 American Association for Cancer Research.
Conflict of interest statement
Conflict of Interests Disclosure Statement
TT Seppälä is the CEO and co-owner of Healthfund Finland; reports an interview honorarium from Boeringer Ingelheim.
DP Ryan is a consultant/advisory board member for MPM Capital, Gritstone Oncology, Oncorus, Maverick Therapeutics, 28/7 Therapeutics, Thrive/Exact Sciences; has equity in MPM Capital, Acworth Pharmaceuticals, and Thrive/Exact Sciences; is a legal consultant for Boeringer Ingelheim; and serves as author for Johns Hopkins University Press, UpToDate, McGraw Hill.
DT Ting is a consultant/advisory board member for Pfizer, ROME Therapeutics, Merrimack Pharmaceuticals, Ventana Roche, Nanostring Technologies, Inc., Foundation Medicine, Inc., and EMD Millipore Sigma, which are not related to this work; is a founder and has equity in PanTher Therapeutics, ROME therapeutics, and TellBio, Inc., which are not related to this work; and has research funding from ACD-Biotechne, PureTech Health LLC, and Ribon Therapeutics, which was not used in this work. DT Ting’s interests were reviewed and are managed by Massachusetts General Hospital and Mass General Brigham in accordance with their conflict-of-interest policies.
Figures
Comment in
-
Patient-Derived Organoid Pharmacotyping Guides Precision Medicine for Pancreatic Cancer.Clin Cancer Res. 2022 Aug 2;28(15):3176-3178. doi: 10.1158/1078-0432.CCR-22-1083. Clin Cancer Res. 2022. PMID: 35617521 Free PMC article.
References
-
- Howlader N, Noone A, Krapcho M, Miller D, Brest A, Yu M, et al. SEER Cancer Statistics Review, 1975–2016 Natl. Cancer Institute. Bethesda, MD. 2019. Available from: https://seer.cancer.gov/csr/1975_2016/
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the united states. Cancer Res 2014;74:2913–21. - PubMed
-
- Conroy T, Hammel P, Hebbar M, Ben Abdelghani M, Wei AC, Raoul JL, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med 2018;379:2395–406. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
