

Phase Ib/II Study of Enzalutamide with Samotolisib (LY3023414) or Placebo in Patients with Metastatic Castration-Resistant Prostate Cancer
- PMID: 35363301
- PMCID: PMC9662871
- DOI: 10.1158/1078-0432.CCR-21-2326
Phase Ib/II Study of Enzalutamide with Samotolisib (LY3023414) or Placebo in Patients with Metastatic Castration-Resistant Prostate Cancer
Abstract
Purpose: To report efficacy and safety of samotolisib (LY3023414; PI3K/mTOR dual kinase and DNA-dependent protein kinase inhibitor) plus enzalutamide in patients with metastatic castration-resistant prostate cancer (mCRPC) following cancer progression on abiraterone.
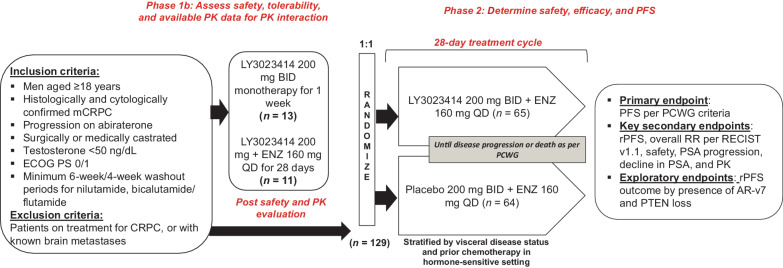
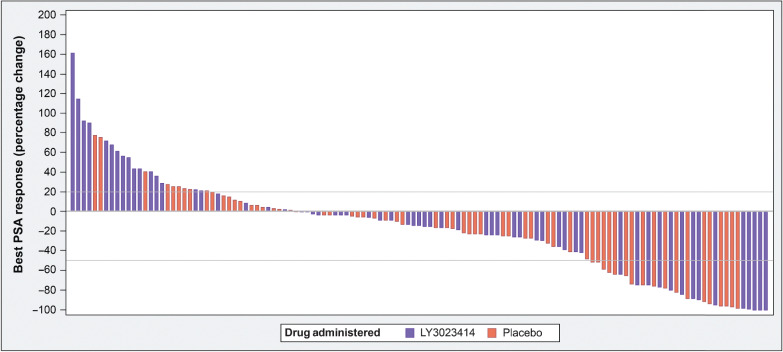
Patients and methods: In this double-blind, placebo-controlled phase Ib/II study (NCT02407054), following a lead-in segment for evaluating safety and pharmacokinetics of samotolisib and enzalutamide combination, patients with advanced castration-resistant prostate cancer with progression on prior abiraterone were randomized to receive enzalutamide (160 mg daily)/samotolisib (200 mg twice daily) or placebo. Primary endpoint was progression-free survival (PFS) assessed by Prostate Cancer Clinical Trials Working Group criteria (PCWG2). Secondary and exploratory endpoints included radiographic PFS (rPFS) and biomarkers, respectively. Log-rank tests assessed treatment group differences.
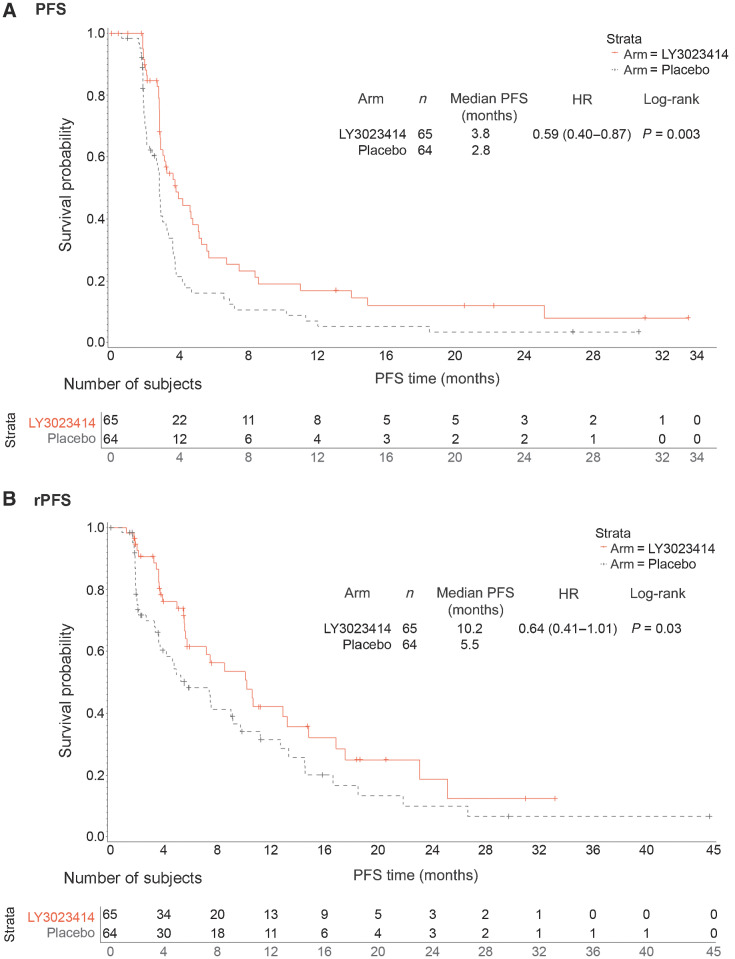
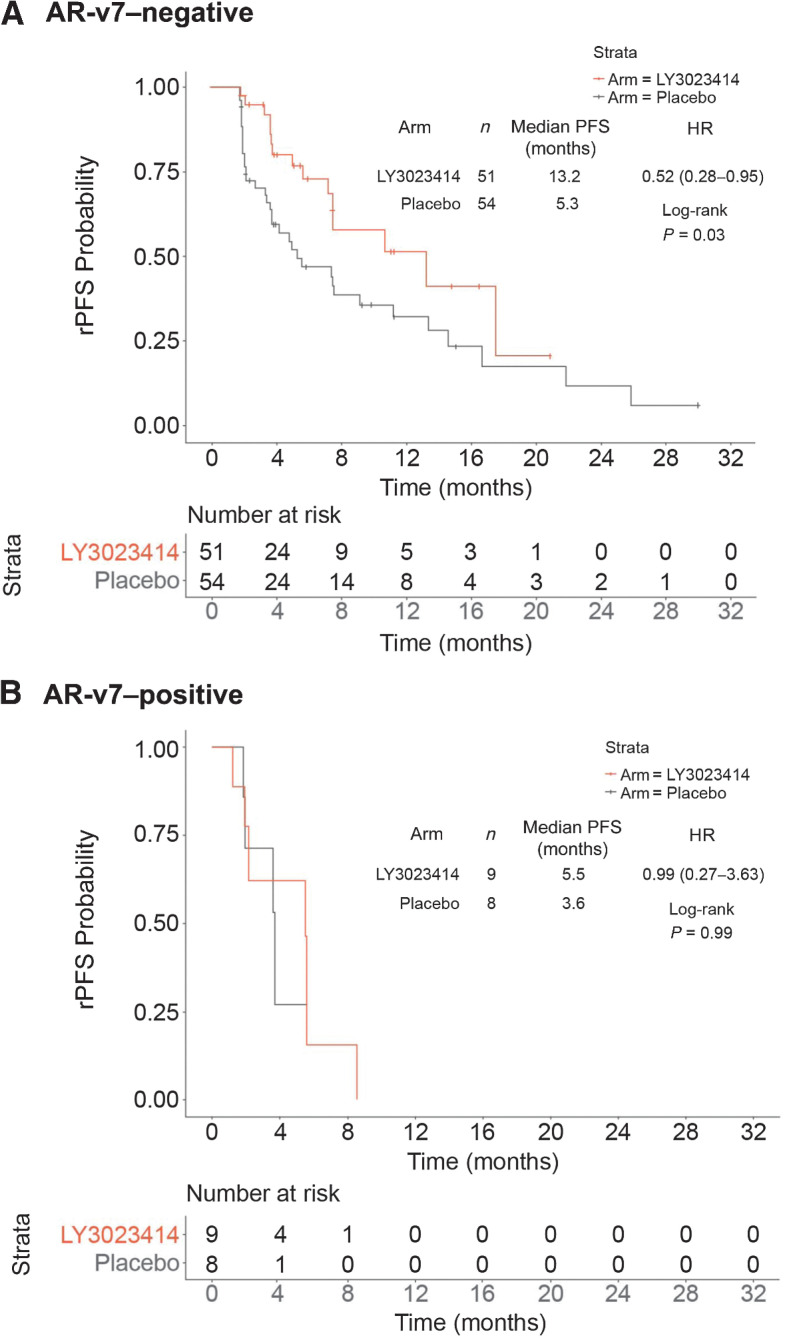
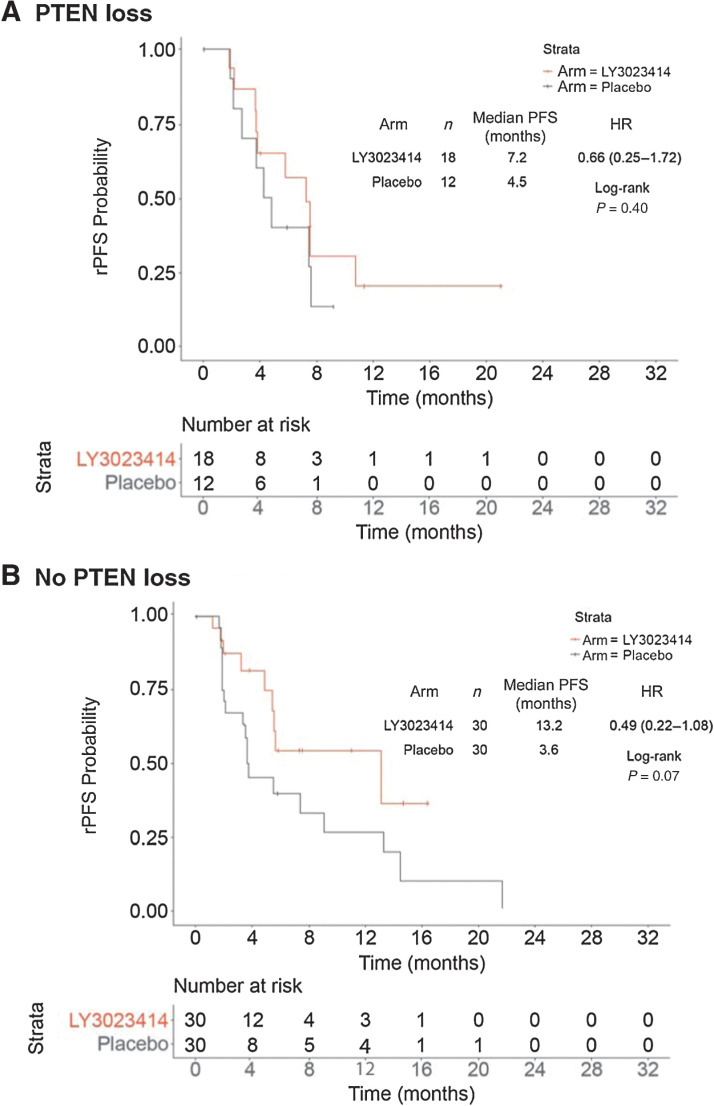
Results: Overall, 13 and 129 patients were enrolled in phase Ib and II, respectively. Dose-limiting toxicity was not reported in patients during phase Ib and mean samotolisib exposures remained in the targeted range despite a 35% decrease when administered with enzalutamide. In phase II, median PCWG2-PFS and rPFS was significantly longer in the samotolisib/enzalutamide versus placebo/enzalutamide arm (3.8 vs. 2.8 months; P = 0.003 and 10.2 vs. 5.5 months; P = 0.03), respectively. Patients without androgen receptor splice variant 7 showed a significant and clinically meaningful rPFS benefit in the samotolisib/enzalutamide versus placebo/enzalutamide arm (13.2 months vs. 5.3 months; P = 0.03).
Conclusions: Samotolisib/enzalutamide has tolerable side effects and significantly improved PFS in patients with mCRPC with cancer progression on abiraterone, and this may be enriched in patients with PTEN intact and no androgen receptor splice variant 7.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–49. - PubMed
-
- Omlin A, Pezaro C, Mukherji D, Mulick Cassidy A, Sandhu S, Bianchini D, et al. Improved survival in a cohort of trial participants with metastatic castration-resistant prostate cancer demonstrates the need for updated prognostic nomograms. Eur Urol 2013;64:300–6. - PubMed
-
- Patrikidou A, Loriot Y, Eymard JC, Albiges L, Massard C, Ileana E, et al. Who dies from prostate cancer? Prostate Cancer Prostatic Dis 2014;17:348–52. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
