

Factors Associated With Severity of COVID-19 Disease in a Multicenter Cohort of People With HIV in the United States, March-December 2020
- PMID: 35364600
- PMCID: PMC9246864
- DOI: 10.1097/QAI.0000000000002989
Factors Associated With Severity of COVID-19 Disease in a Multicenter Cohort of People With HIV in the United States, March-December 2020
Abstract
Background: Understanding the spectrum of COVID-19 in people with HIV (PWH) is critical to provide clinical guidance and risk reduction strategies.
Setting: Centers for AIDS Research Network of Integrated Clinic System, a US multisite clinical cohort of PWH in care.
Methods: We identified COVID-19 cases and severity (hospitalization, intensive care, and death) in a large, diverse HIV cohort during March 1, 2020-December 31, 2020. We determined predictors and relative risks of hospitalization among PWH with COVID-19, adjusted for disease risk scores.
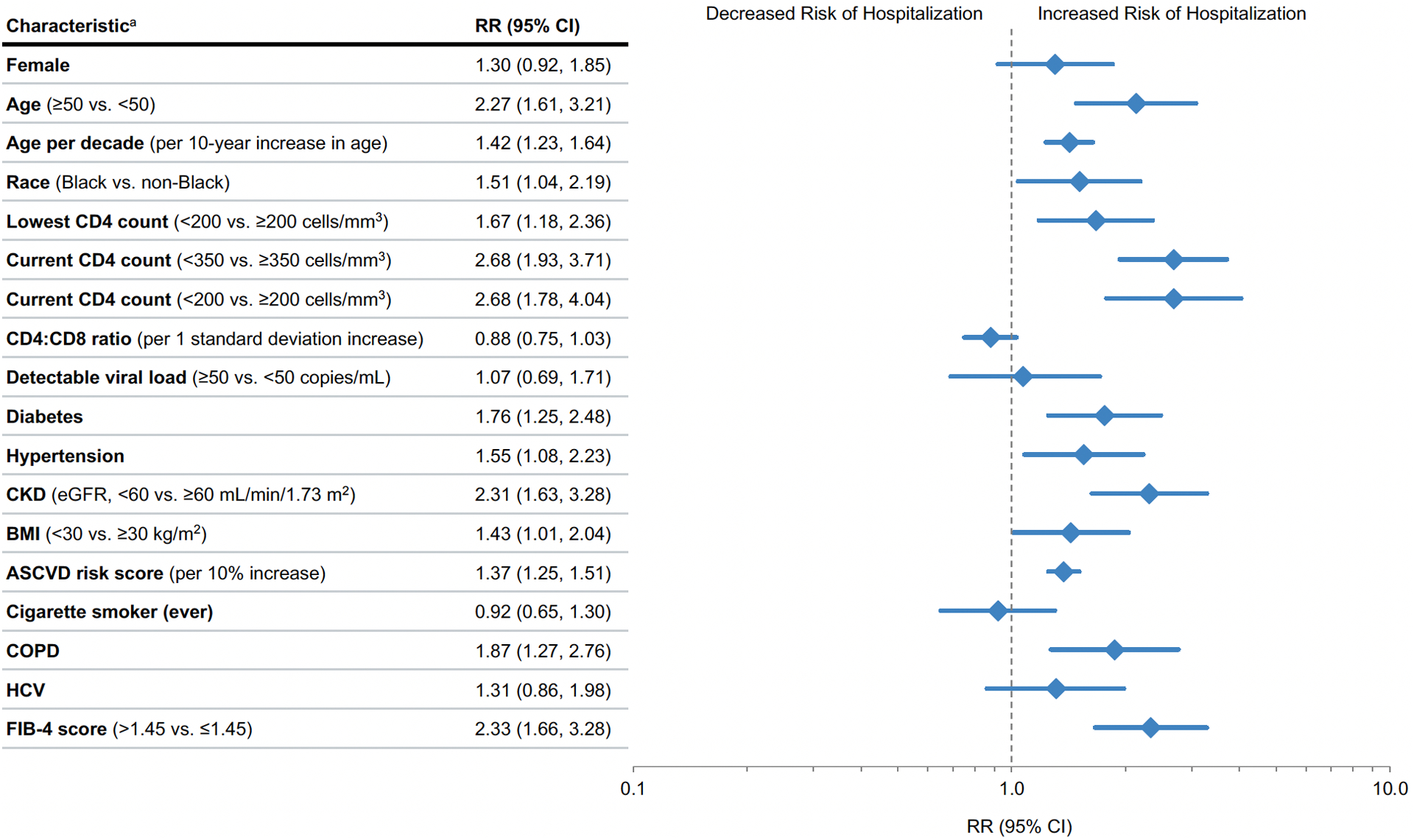
Results: Of 16,056 PWH in care, 649 were diagnosed with COVID-19 between March and December 2020. Case fatality was 2%; 106 (16.3%) were hospitalized, and 12 died. PWH with current CD4 count <350 cells/mm 3 [aRR 2.68; 95% confidence interval (CI): 1.93 to 3.71; P < 0.001] or lowest recorded CD4 count <200 cells/mm 3 (aRR 1.67; 95% CI: 1.18 to 2.36; P < 0.005) had greater risks of hospitalization. HIV viral load and antiretroviral therapy status were not associated with hospitalization, although most of the PWH were suppressed (86%). Black PWH were 51% more likely to be hospitalized with COVID-19 compared with other racial/ethnic groups (aRR 1.51; 95% CI: 1.04 to 2.19; P = 0.03). Chronic kidney disease, chronic obstructive pulmonary disease, diabetes, hypertension, obesity, and increased cardiovascular and hepatic fibrosis risk scores were associated with higher hospitalization risk. PWH who were older, not on antiretroviral therapy, and with current CD4 count <350 cells/mm 3 , diabetes, and chronic kidney disease were overrepresented among PWH who required intubation or died.
Conclusions: PWH with CD4 count <350 cells/mm 3 , and a history of CD4 count <200 cells/mm 3 , have a clear excess risk of severe COVID-19, accounting for comorbidities associated with severe outcomes. PWH with these risk factors should be prioritized for COVID-19 vaccination and early treatment and monitored closely for worsening illness.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Update of
-
Factors associated with severity of COVID-19 disease in a multicenter cohort of people with HIV in the United States, March-December 2020.medRxiv [Preprint]. 2021 Oct 18:2021.10.15.21265063. doi: 10.1101/2021.10.15.21265063. medRxiv. 2021. Update in: J Acquir Immune Defic Syndr. 2022 Aug 1;90(4):369-376. doi: 10.1097/QAI.0000000000002989. PMID: 34704092 Free PMC article. Updated. Preprint.
References
-
- Armstrong WS, Agwu AL, Barrette EP, et al. Innovations in Human Immunodeficiency Virus (HIV) Care Delivery During the Coronavirus Disease 2019 (COVID-19) Pandemic: Policies to Strengthen the Ending the Epidemic Initiative-A Policy Paper of the Infectious Diseases Society of America and the HIV Medicine Association. Clin Infect Dis. Jan 23 2021;72(1):9–14. doi:10.1093/cid/ciaa1532 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AI027767/AI/NIAID NIH HHS/United States
- P30 AI094189/AI/NIAID NIH HHS/United States
- K24 AI145806/AI/NIAID NIH HHS/United States
- UL1 TR001442/TR/NCATS NIH HHS/United States
- K23 AI140918/AI/NIAID NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- R01 DA047045/DA/NIDA NIH HHS/United States
- P30 AI060354/AI/NIAID NIH HHS/United States
- P30 AI036219/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- P30 AI036214/AI/NIAID NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
