

Extremely premature infants born at 23-25 weeks gestation are at substantial risk for pulmonary hypertension
- PMID: 35365772
- PMCID: PMC9184271
- DOI: 10.1038/s41372-022-01374-w
Extremely premature infants born at 23-25 weeks gestation are at substantial risk for pulmonary hypertension
Abstract
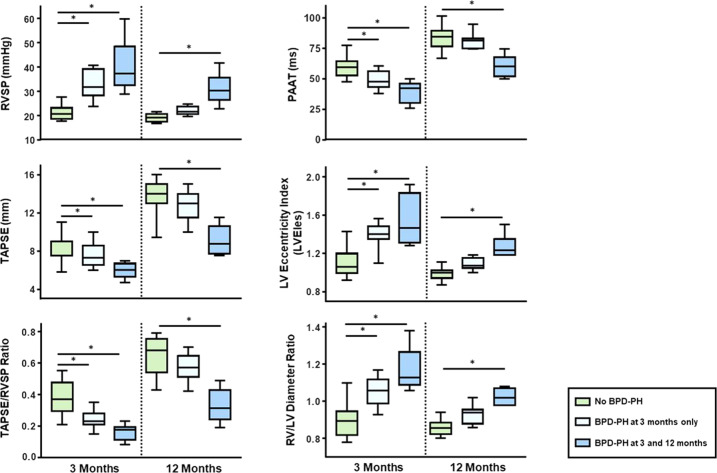
Objective: Extremely low gestational age newborns (ELGANs) represent an especially vulnerable population. Herein, we aimed to determine incidence and severity of pulmonary hypertension associated with bronchopulmonary dysplasia (BPD-PH) in extremely immature ELGANs (gestational age: 230/6-256/7 weeks).
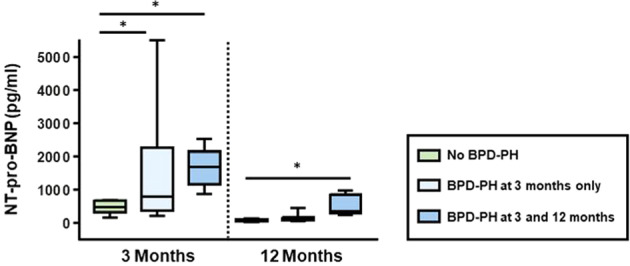
Methods: In this prospective observational cohort study, we assessed BPD-PH by means of several echocardiography markers and serum N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels at 3 and 12 months of chronological age. In addition, we analyzed incidence and efficacy of pharmacologic treatment for BPD-PH.
Results: At 3 months 15/34 ELGANs had echocardiographic evidence of BPD-PH, while at 12 months of age 6/34 still had PH. PH-targeted therapy consisted of sildenafil monotherapy in 11 and dual oral combination therapy (sildenafil and macitentan) in four ELGANs at 3 and 12 months.
Conclusion: 44% (15/34) of ELGANs developed BPD-PH. All received PH-targeted pharmacotherapy at 3 months, leading to hemodynamic improvements at 12 months in most infants.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Comment in
-
Reply.J Pediatr. 2022 Nov;250:110-112. doi: 10.1016/j.jpeds.2022.07.051. Epub 2022 Aug 6. J Pediatr. 2022. PMID: 35944715 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
