

Treatment of open-angle glaucoma and ocular hypertension with preservative-free tafluprost/timolol fixed-dose combination therapy: 6 case reports and clinical outcomes
- PMID: 35366846
- PMCID: PMC8977001
- DOI: 10.1186/s12886-022-02361-7
Treatment of open-angle glaucoma and ocular hypertension with preservative-free tafluprost/timolol fixed-dose combination therapy: 6 case reports and clinical outcomes
Abstract
Background: Treatment of open angle glaucoma (OAG) and/or ocular hypertension (OHT) focuses on achievement of target intraocular pressure (IOP), with the objective of slowing disease progression. However, ocular surface health is an important consideration in the optimization of treatment. We report 6 patient cases in which enhanced IOP control was achieved following appropriate management of ocular surface inflammation and a therapeutic switch to the preservative-free (PF) tafluprost (0.0015%)/timolol (0.5%) fixed-dose combination (FC).
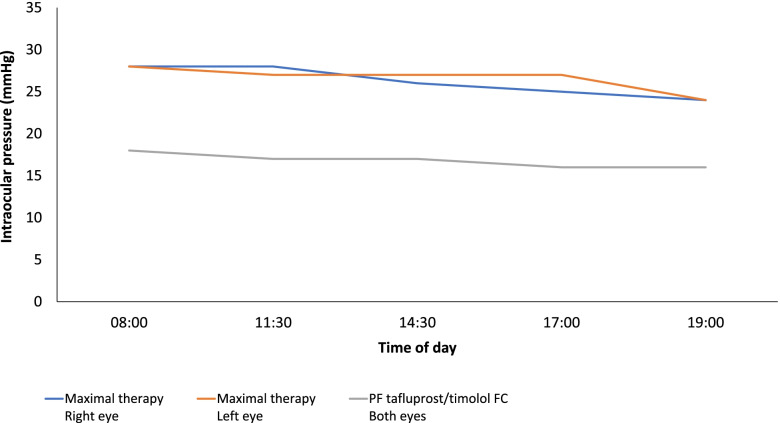
Case presentation: Six patient cases, aged 48-74 years, presented with OAG or OHT. Each patient had signs and symptoms of ocular surface disease (OSD). Cases 1-3 were each receiving maximal medical therapy for OAG; regimens comprising prostaglandin analogue (PGA), β-blocker, carbonic anhydrase inhibitor (CAI) and α-2 agonist agents (including treatments containing preservative agent). Cases 1 and 2 reported IOP values ≥23 mmHg in each eye, and wide IOP fluctuations were identified when reviewing patient data concerning case 3 (11-20 mmHg). Maximal therapy was ceased and PF tafluprost/timolol FC was initiated, after which the signs and symptoms of OSD were improved and IOP was reduced (≤18 mmHg for cases 1-3) and stabilized. Cases 4 and 5 were diagnosed with OAG and case 6 had OHT. Each had symptoms and signs of OSD and were treated with a preserved PGA monotherapy (latanoprost 0.005% or bimatoprost 0.03%). At presentation, IOP was 24 mmHg in both eyes (case 4), ≥18 mmHg (case 5) and ≥ 22 mmHg (case 6). Following a switch to the PF tafluprost/timolol FC, OSD symptoms were improved and IOP was 14 mmHg (both eyes; case 4), ≤14 mmHg (case 5) and 16 mmHg (both eyes; case 6).
Conclusions: In addition to IOP-lowering efficacy, approaches to the management of OAG and OHT should consider the impact of treatment tolerability and the susceptibility of these patients to OSD. The presence of ocular surface inflammation appears to be detrimental to adherence and therefore to the effectiveness of topical medications. Addressing OSD through the use of PF FC formations, such as the PF tafluprost/timolol FC, reduces exposure to potentially toxic agents and facilitates improvements in IOP control.
Keywords: BAK; Benzalkonium chloride; Case report; Fixed-dose combination; Ocular hypertension; Ocular surface disease; Open-angle glaucoma; Preservative-free topical medication; Tafluprost/timolol.
© 2022. The Author(s).
Conflict of interest statement
Ejaz Ansari has received lecturing fees from Santen and Théa.
Shankar Chappiti has received lecture fees and educational grant funding from Santen UK, Glaucoma Trainer fees from Novartis UK and lecture fees from Medicom Healthcare UK.
Jasna Pavicic-Astalos has received consultancy and lecturing fees from TheaPamex, Santen and Allergan.
Juan Carlos Pinto-Bonilla has no relevant financial declarations.
Ivano Riva declares honoraria and congress expenses from Allergan, Santen, Visufarma, SOOFT/Glaucoom, SIFI.
Matteo Sacchi has no relevant financial declarations.
Figures



References
-
- International Council of Ophthalmology. Guidelines for glaucoma care. 2016. https://icoph.org/eye-care-delivery/glaucoma/ Accessed 21 January 2022.
-
- European Glaucoma Society. Terminology and guidelines for glaucoma, 5th Edition. 2020. Available at: https://www.eugs.org/eng/guidelines.asp Accessed 21 January 2022.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
