

doi: 10.1093/europace/euac038.
How to use digital devices to detect and manage arrhythmias: an EHRA practical guide
Affiliations
- PMID: 35368065
- PMCID: PMC11636571
- DOI: 10.1093/europace/euac038
Item in Clipboard
How to use digital devices to detect and manage arrhythmias: an EHRA practical guide
Europace.
.
Erratum in
-
Corrigendum to: How to use digital devices to detect and manage arrhythmias: an EHRA practical guide.Europace. 2022 Jul 15;24(6):1005. doi: 10.1093/europace/euac067. Europace. 2022. PMID: 35527708 No abstract available.
-
Corrigendum to: How to use digital devices to detect and manage arrhythmias: an EHRA practical guide.Europace. 2023 Feb 16;25(2):486. doi: 10.1093/europace/euac227. Europace. 2023. PMID: 36517218 Free PMC article. No abstract available.
No abstract available
Figures
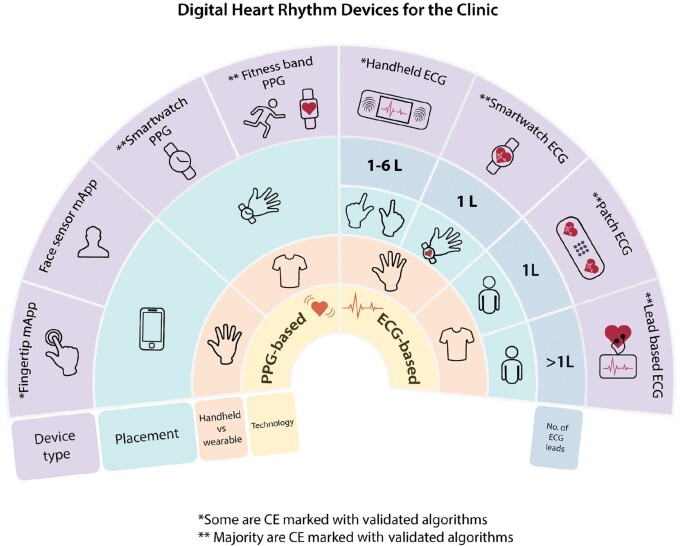
Overview of digital heart rhythm devices for the clinic. Suggest reading the figure from the inner circle—devices have been divided into devices that provide photoplethysmography (PPG) or electrocardiogram (ECG), followed by the mode of handheld or wearable, and then placement on the body, number of leads, and device type. */**Please see Table 2 for further details. ECG, electrocardiogram; L, lead; mApp, mobile App; PPG, photoplethysmography.
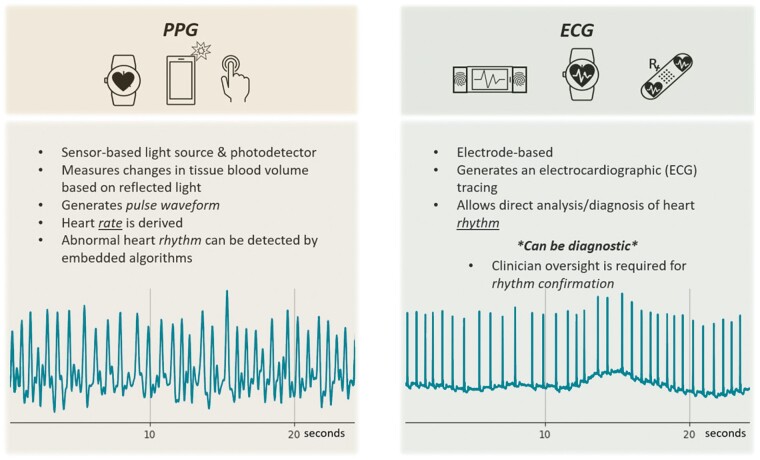
Comparison of photoplethysmography (PPG) vs. electrogram (ECG)-based techniques. In the lower part of the figure an example of a registration from a patient with atrial fibrillation is shown.
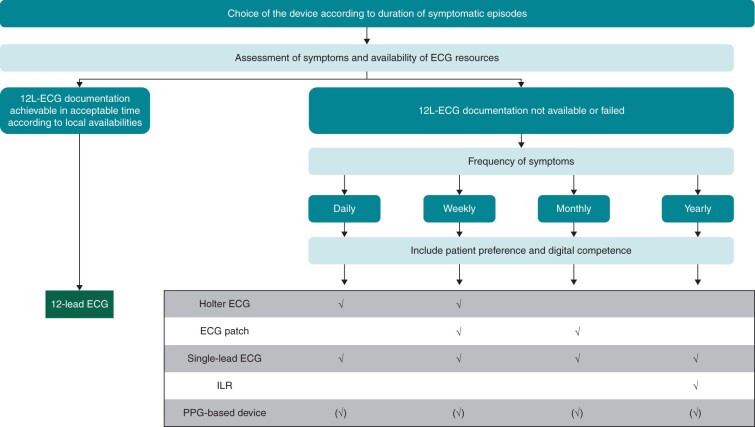
Choice of ECG device in symptomatic patient. If possible, subject to availability and duration of symptoms a 12-lead ECG should be achieved to evaluate symptomatic arrhythmias. In case of difficulties achieving a 12-lead ECG during symptomatic episodes, assess the frequency of symptoms and patient preference prior to choosing long-term ECG device for heart rhythm monitoring. (✓) possible use; 12 L, 12 lead; ECG, electrocardiogram; ILR, implantable loop recorder.
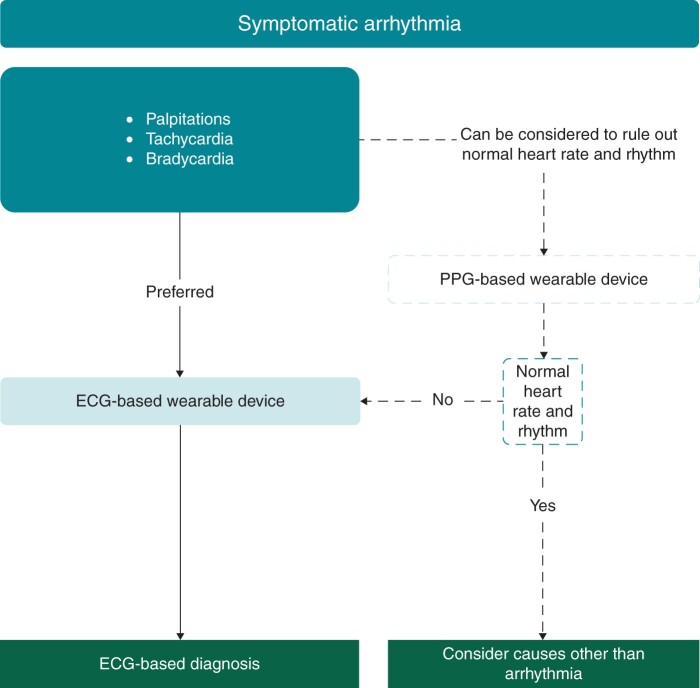
Suggested workflow for the management of symptomatic arrhythmias.
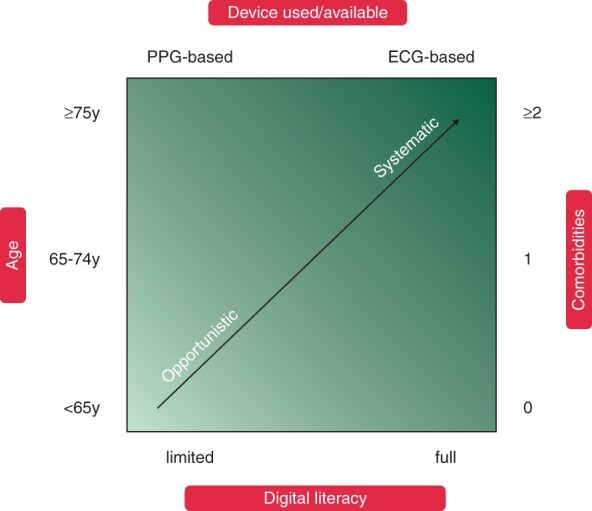
Considerations for atrial fibrillation screening programme (systematic or opportunistic) and digital device based on patient age, comorbidities, and digital literacy.
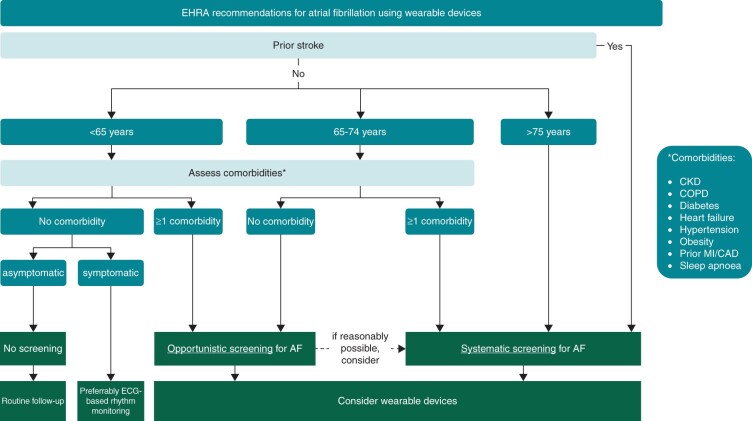
EHRA suggestions for screening for atrial fibrillation using digital devices. For patients with a prior stroke, a systematic screening approach for AF should always be implemented, preferably immediately after the event. As age is the most important risk factor for stroke, suggestions are based on age, with individuals at or above 75 at highest risk. For younger individuals, screening might still be warranted based on their risk factors as per the CHA2DS2-VASc score, and in addition for individuals at higher risk such as patients with CKD (chronic kidney disease), COPD (chronic obstructive pulmonary disease), obesity, and sleep apnoea., AF, atrial fibrillation; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; ECG, electrocardiogram; MI, myocardial infarction.
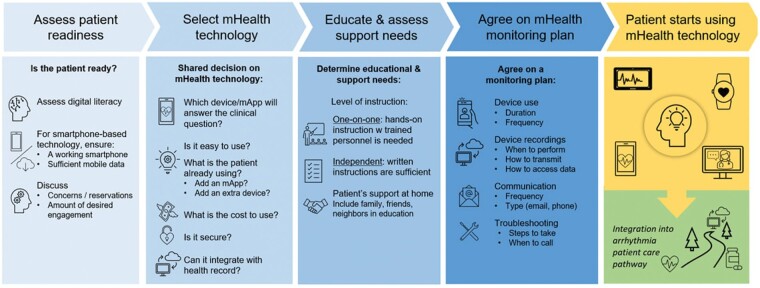
Patient engagement.
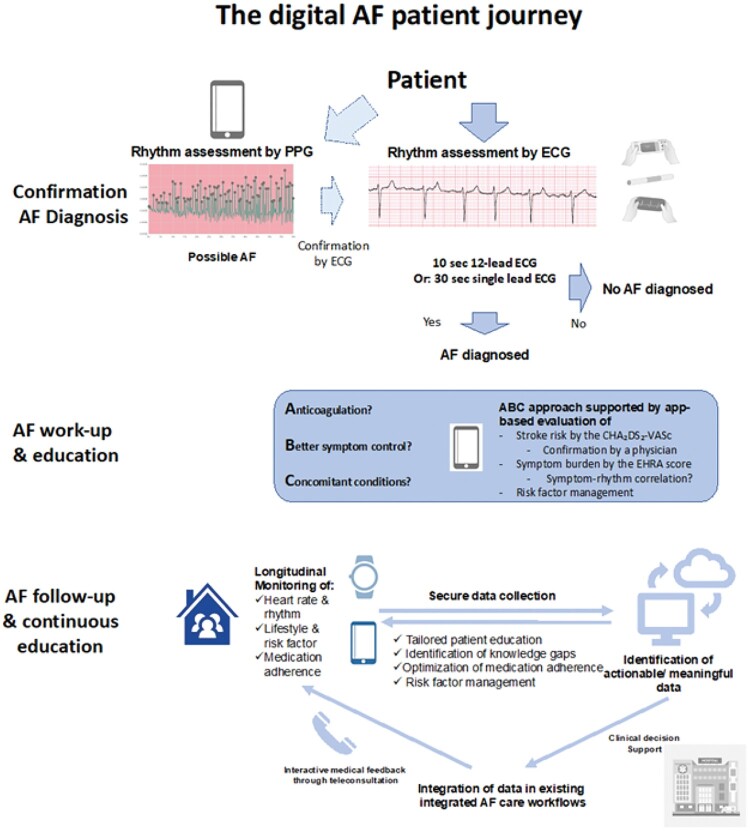
The potential uses of digital devices in patients with atrial fibrillation.
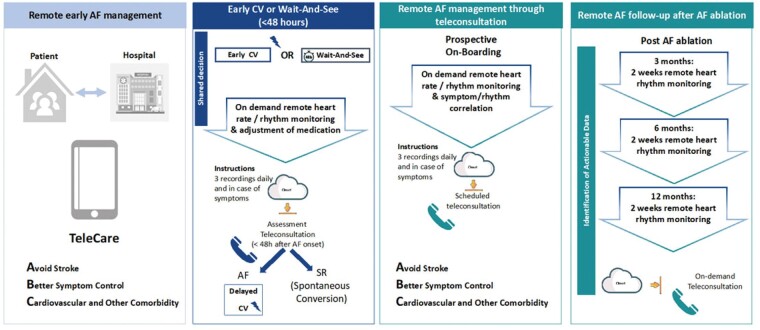
Practical examples of digital AF management. Note that for Panels 2–4 randomized controlled trials are still lacking, and these should be views as examples of ongoing practical applications of digital tools. For all on demand remote heart rate/rhythm monitoring, an experienced physician should verify the findings by the device.
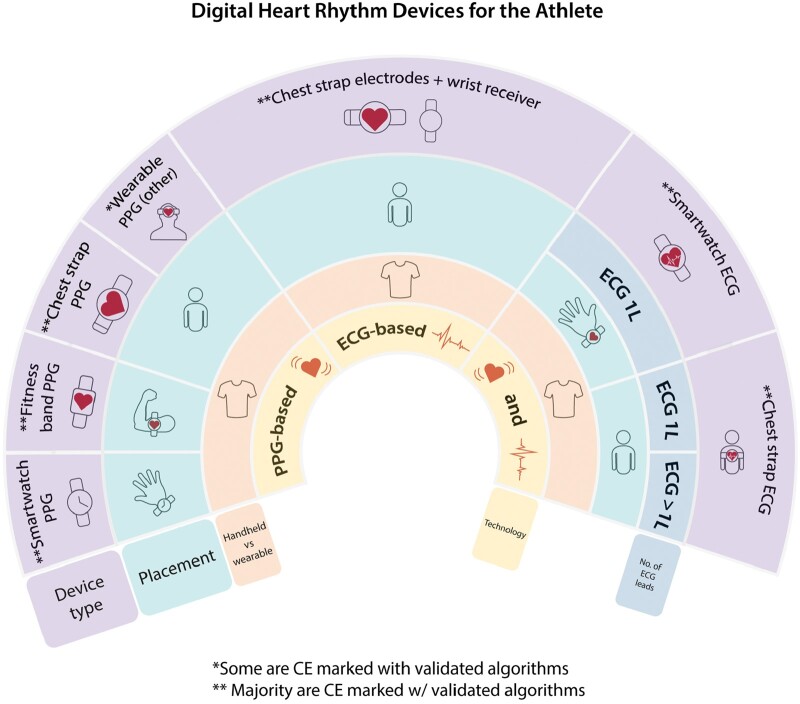
Overview of digital devices for athletes.
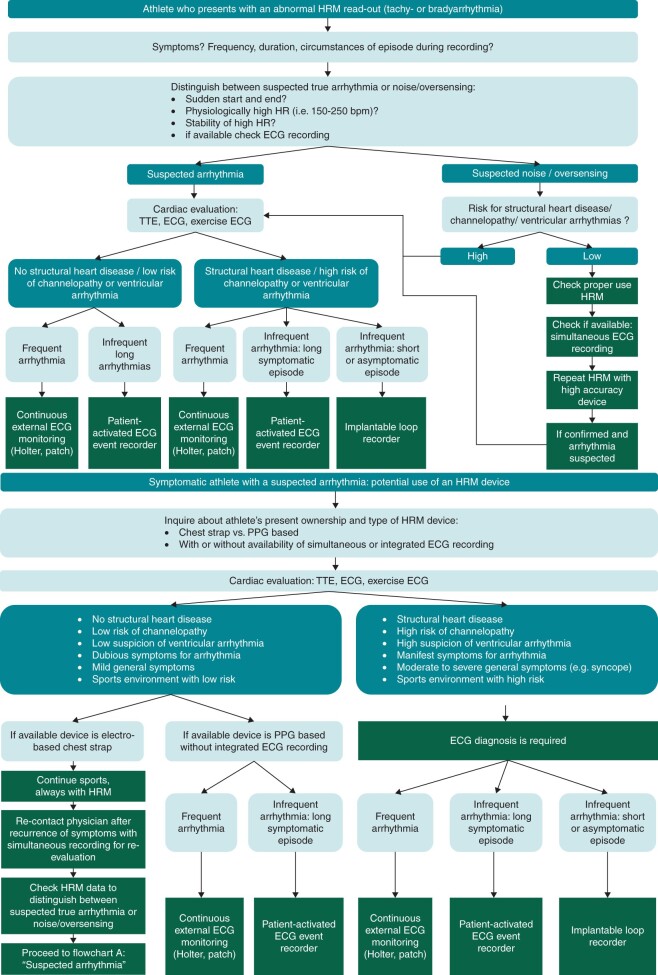
Flowcharts diagnostic scenarios in athletes with (A) abnormal heart rate monitor (HRM) readings and/or (B) suspected arrhythmias. bpm, beats per minute; ECG, electrocardiogram; HR, heart rate; HRM, heart rate monitor; PPG, photoplethysmography; TTE, transthoracic echocardiogram.
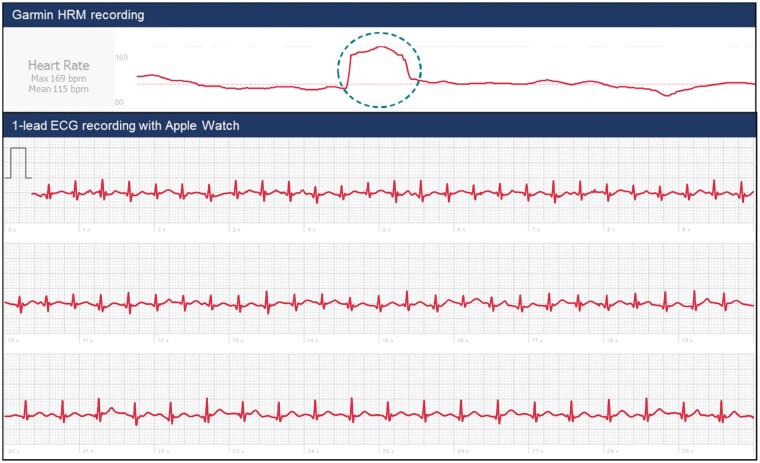
Athlete with sudden heart rate accelerations documented on heart rate monitoring device. An athlete (48-year old male) presented to the outpatient clinic with palpitations during cycling exercise with heart rate accelerations from 120 to 180 b.p.m. without any clear triggers. His chest strap band (Garmin Edge 1030) output showed a sudden start and onset of the episodes, which coincided with subjective palpitations. The combination of known chest strap accuracy and symptoms made an arrhythmia likely. Since cardiac evaluation ruled out structural heart disease, and the episodes were of longer duration (see Flowchart A), patient-activated ECG recording was deemed necessary. The patient also happened to have an Apple Watch 4 and was instructed to record an ECG on recurrence of symptoms and/or heart rate accelerations (see Flowchart B, left-sided scenario). He subsequently presented with a recording taken after an heart rate jump and complaints of palpitations (blue dotted circle), which confirmed an SVT (which terminated at the end of recording).
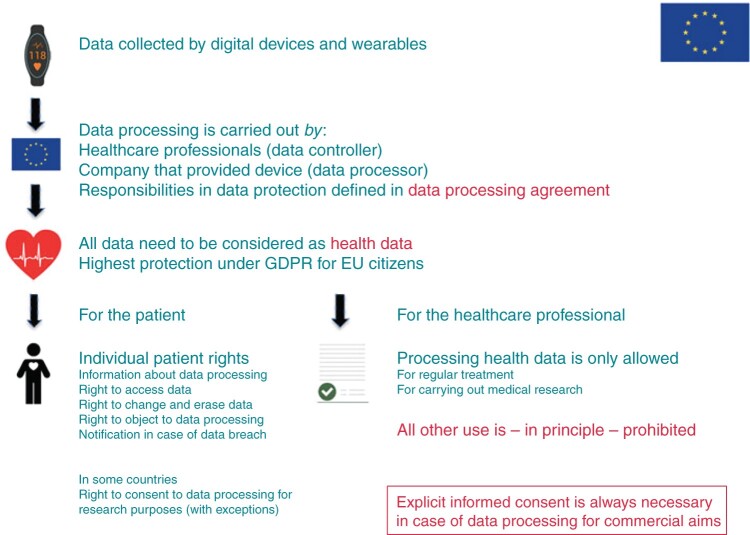
Processing health data.
References
-
- Manninger M, Zweiker D, Svennberg E, Chatzikyriakou S, Pavlovic N, Zaman JAB et al. Current perspectives on wearable rhythm recordings for clinical decision-making: the wEHRAbles 2 survey. Europace 2021;23:1106–1113. - PubMed
-
- Albert DE. Performance of hand-held electrocardiogram devices to detect atrial fibrillation in a cardiology and geriatric ward setting. Europace 2017;19:1408. - PubMed
-
- Brito R, Mondouagne LP, Stettler C, Combescure C, Burri H. Automatic atrial fibrillation and flutter detection by a handheld ECG recorder, and utility of sequential finger and precordial recordings. J Electrocardiol 2018;51:1135–40. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
