

Focal Segmental Glomerulosclerosis, Risk Factors for End Stage Kidney Disease, and Response to Immunosuppression
- PMID: 35368810
- PMCID: PMC8785735
- DOI: 10.34067/KID.0006172020
Focal Segmental Glomerulosclerosis, Risk Factors for End Stage Kidney Disease, and Response to Immunosuppression
Abstract
Background: FSGS is a heterogeneic glomerular disease. Risk factors for kidney disease ESKD and the effect of immunosuppression treatment (IST) has varied in previously published cohorts. These cohorts were limited by relatively small case numbers, short follow-up, lack of racial/ethnic diversity, a mix of adult and pediatric patients, lack of renin-angiotensin-aldosterone system (RAAS) inhibition, or lack of subgroup analysis of IST.
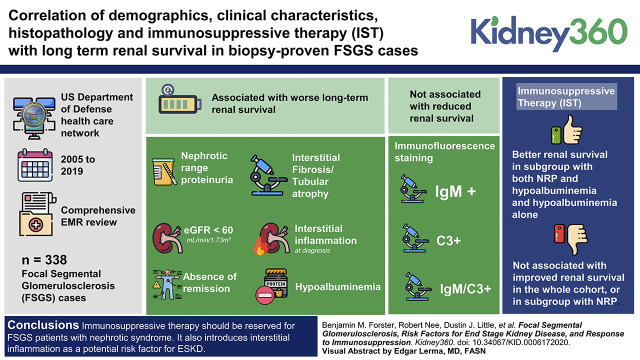
Methods: We compared demographics, clinical characteristics, histopathology, and IST to long-term renal survival in a large, ethnically diverse, adult cohort of 338 patients with biopsy-proven FSGS with long-term follow-up in the era of RAAS inhibition using data from the US Department of Defense health care network.
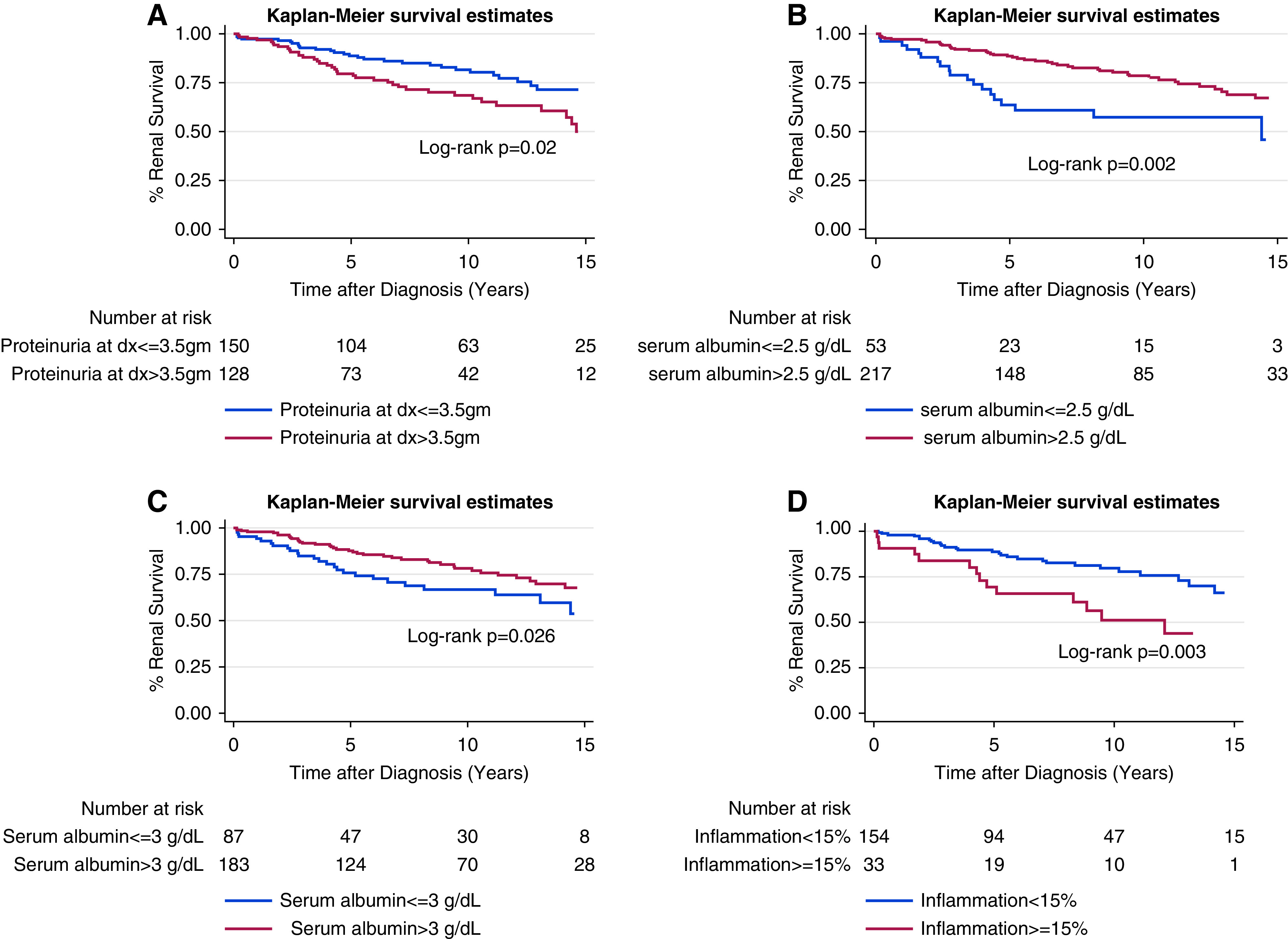
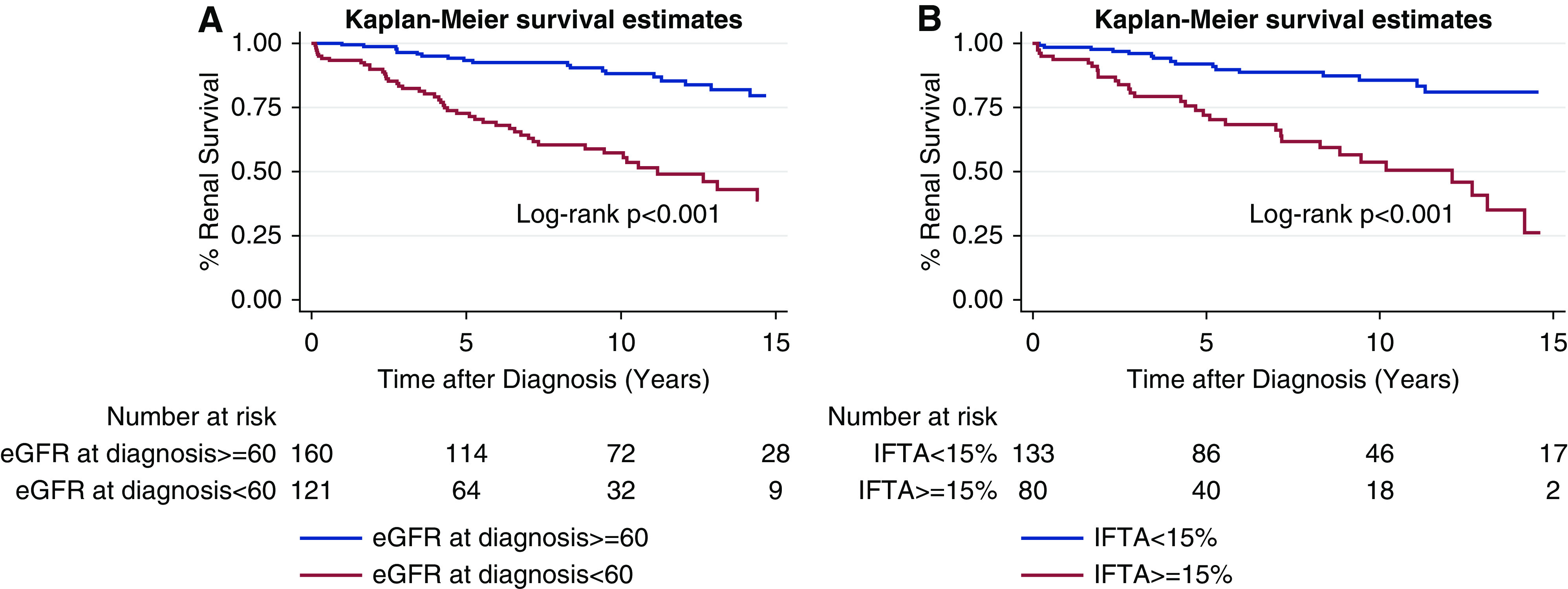
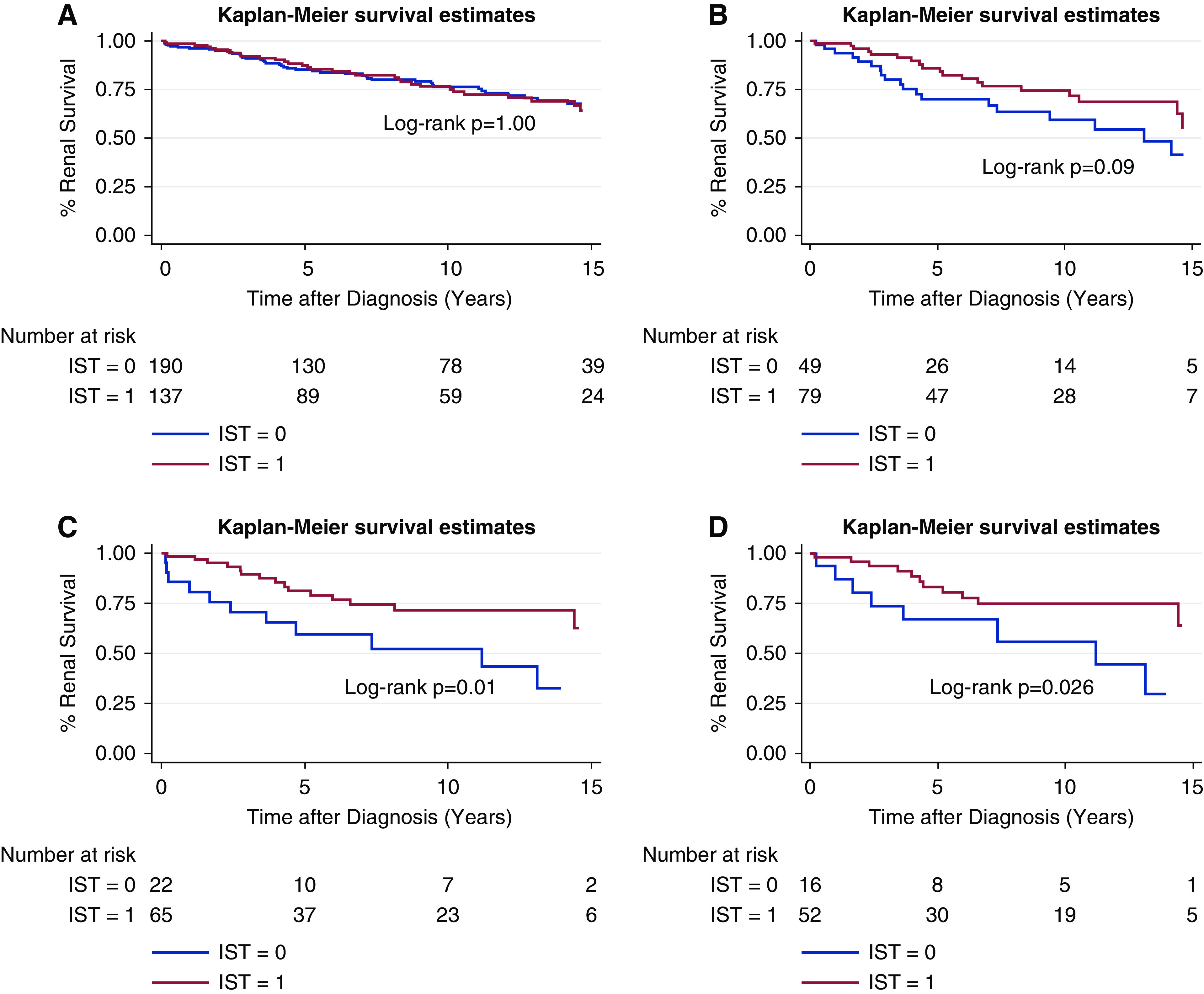
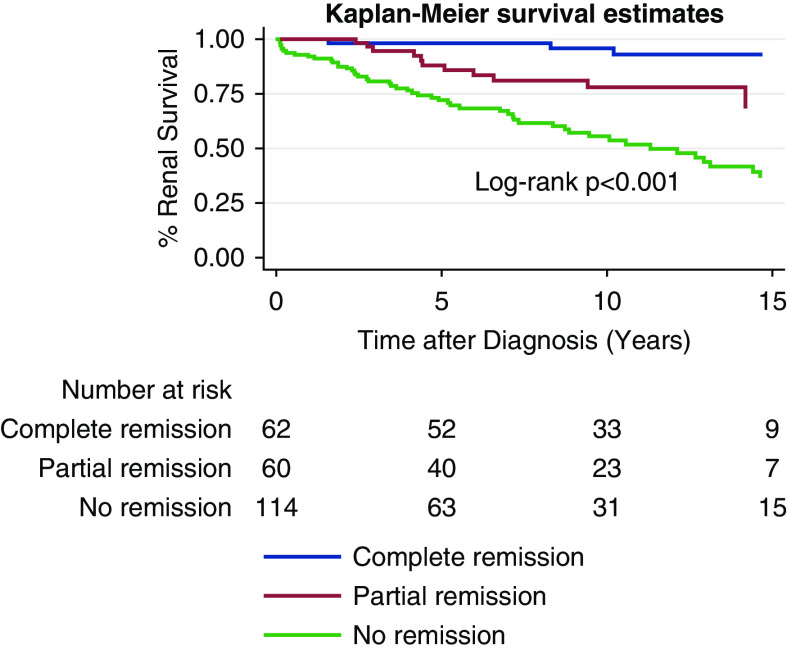
Results: Multivariate analysis showed that nephrotic-range proteinuria (NRP), eGFR <60 ml/min per 1.73 m2, hypoalbuminemia, interstitial fibrosis and tubular atrophy, and interstitial inflammation at diagnosis and the absence of remission were all associated with worse long-term renal survival. IgM, C3, and a combination of IgM/C3 immunofluorescence staining were not associated with reduced renal survival. IST was not associated with improved renal survival in the whole cohort, or in a subgroup with NRP. However, IST was associated with better renal survival in a subgroup of patients with FSGS with both NRP and hypoalbuminemia and hypoalbuminemia alone.
Conclusions: Our study suggests that IST should be reserved for patients with FSGS and nephrotic syndrome. It also introduces interstitial inflammation as a potential risk factor for ESKD and does not support the proposed pathogenicity of IgM and complement activation.
Keywords: end stage kidney disease; estimated glomerular filtration rate; focal segmental glomerulosclerosis; glomerular and tubulointerstitial diseases; immunosuppression; proteinuria; renal survival; risk factors.
Copyright © 2021 by the American Society of Nephrology.
Conflict of interest statement
D. Little and P. Greasley both work for AstraZeneca. They have no significant financial arrangements to produce or sell products that are the subject of the studies reported in this manuscript. All remaining authors have nothing to disclose.
Figures
References
-
- Troyanov S, Wall CA, Miller JA, Scholey JW, Cattran DC; Toronto Glomerulonephritis Registry Group: Focal and segmental glomerulosclerosis: Definition and relevance of a partial remission. J Am Soc Nephrol 16: 1061–1068, 2005 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
