

Estimating Kidney Failure Risk Using Electronic Medical Records
- PMID: 35369014
- PMCID: PMC8786004
- DOI: 10.34067/KID.0005592020
Estimating Kidney Failure Risk Using Electronic Medical Records
Abstract
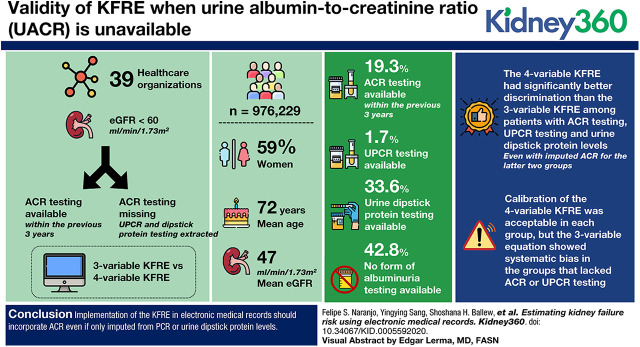
Background: The four-variable kidney failure risk equation (KFRE) is a well-validated tool for patients with GFR <60 ml/min per 1.73 m2 and incorporates age, sex, GFR, and urine albumin-creatinine ratio (ACR) to forecast individual risk of kidney failure. Implementing the KFRE in electronic medical records is challenging, however, due to low ACR testing in clinical practice. The aim of this study was to determine, when ACR is missing, whether to impute ACR from protein-to-creatinine ratio (PCR) or dipstick protein for use in the four-variable KFRE, or to use the three-variable KFRE, which does not require ACR.
Methods: Using electronic health records from OptumLabs Data Warehouse, patients with eGFR <60 ml/min per 1.73 m2 were categorized on the basis of the availability of ACR testing within the previous 3 years. For patients missing ACR, we extracted urine PCR and dipstick protein results, comparing the discrimination of the three-variable KFRE (age, sex, GFR) with the four-variable KFRE estimated using imputed ACR from PCR and dipstick protein levels.
Results: There were 976,299 patients in 39 health care organizations; 59% were women, the mean age was 72 years, and mean eGFR was 47 ml/min per 1.73 m2. The proportion with ACR testing was 19% within the previous 3 years. An additional 2% had an available PCR and 36% had a dipstick protein; the remaining 43% had no form of albuminuria testing. The four-variable KFRE had significantly better discrimination than the three-variable KFRE among patients with ACR testing, PCR testing, and urine dipstick protein levels, even with imputed ACR for the latter two groups. Calibration of the four-variable KFRE was acceptable in each group, but the three-variable equation showed systematic bias in the groups that lacked ACR or PCR testing.
Conclusions: Implementation of the KFRE in electronic medical records should incorporate ACR, even if only imputed from PCR or urine dipstick protein levels.
Keywords: albuminuria; chronic kidney disease; electronic health records; kidney failure.
Copyright © 2021 by the American Society of Nephrology.
Conflict of interest statement
A. Levey reports receiving research funding from grants and contracts paid to Tufts Medical Center from the National Institutes of Health (NIH) and the National Kidney Foundation (NKF); contracts to paid from AstraZeneca (DSMB); and reports receiving honoraria from academic medical centers for visiting professorships. J. Coresh reports consultancy agreements with Healthy.io, Kaleido, and Ultragenyx; having an ownership interest in Healthy.io; reports receiving research funding from the NKF and the NIH; and reports being a scientific advisor or member of Healthy.io and NKF. M. Grams reports receiving honoraria from academic institutions for giving grand rounds and American Society of Nephrology for Young Investigator Award; reports being a scientific advisor or member of AJKD, CJASN, and the JASN Editorial Fellowship Committee, NKF Scientific Advisory Board, KDIGO Executive Committee, USRDS Scientific Advisory Board; reports having other interests/relationships with the NKF, which receives funding from Abbvie, Relypsa, and Thrasos; reports receiving travel support from Dialysis Clinics, Inc. to speak at the annual meeting and KDIGO for participation in scientific meetings and the executive committee. S. Dunning reports having an ownership interest in UnitedHealth Group. All remaining authors have nothing to disclose.
References
-
- Matsushita K, Coresh J, Sang Y, Chalmers J, Fox C, Guallar E, Jafar T, Jassal SK, Landman GWD, Muntner P, Roderick P, Sairenchi T, Schöttker B, Shankar A, Shlipak M, Tonelli M, Townend J, van Zuilen A, Yamagishi K, Yamashita K, Gansevoort R, Sarnak M, Warnock DG, Woodward M, Ärnlöv J; CKD Prognosis Consortium: Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: A collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol 3: 514–525, 2015. 10.1016/S2213-8587(15)00040-6 - DOI - PMC - PubMed
-
- Tangri N, Grams ME, Levey AS, Coresh J, Appel LJ, Astor BC, Chodick G, Collins AJ, Djurdjev O, Elley CR, Evans M, Garg AX, Hallan SI, Inker LA, Ito S, Jee SH, Kovesdy CP, Kronenberg F, Heerspink HJL, Marks A, Nadkarni GN, Navaneethan SD, Nelson RG, Titze S, Sarnak MJ, Stengel B, Woodward M, Iseki K; CKD Prognosis Consortium: Multinational assessment of accuracy of equations for predicting risk of kidney failure: A meta-analysis [published correction appears in JAMA 315: 822, 2016 10.1001/jama.2016.0342]. JAMA 315: 164–174, 2016. 10.1001/jama.2015.18202 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
