

WiSE CRT Is Beneficial for Heart Failure Patients as a Rescue Therapy: Evidence From a Meta-Analysis
- PMID: 35369306
- PMCID: PMC8964787
- DOI: 10.3389/fcvm.2022.823797
WiSE CRT Is Beneficial for Heart Failure Patients as a Rescue Therapy: Evidence From a Meta-Analysis
Abstract
Background: Leadless endocardial left ventricular (LV) pacing resynchronization therapy is a novel solution for patients with heart failure (HF) in whom conventional cardiac resynchronization therapy (CRT) failed.
Methods: PubMed and the Cochrane Library were searched for relevant cohort studies. Clinical outcomes of interest such as ejection fraction (EF), QRS duration (QRSd), and left ventricular end-systolic volume (LVESV) were extracted and analyzed.
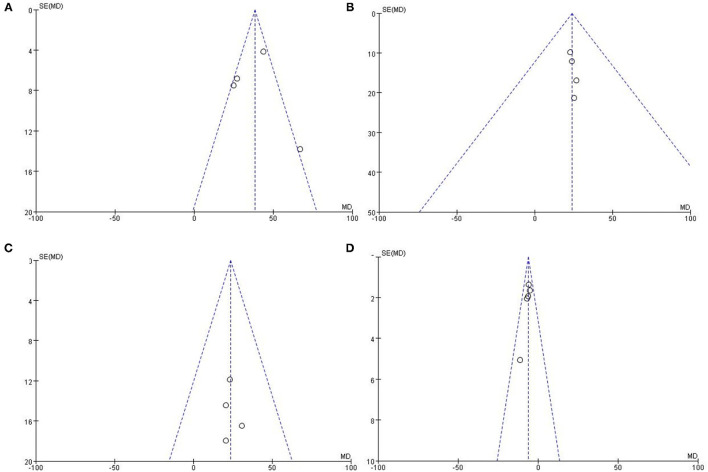
Results: Five studies involving 175 HF patients for WiSE CRT were included, and patients were followed-up for 6 months. The implanted success rate ranged from 76.5 to 100%. WiSE CRT resulted in significantly narrower QRSd [mean difference (MD): -38.21 ms, 95% confidence interval (CI): -44.36 to -32.07, p < 0.001], improved left ventricular ejection fraction (MD: 6.07%, 95% CI: 4.43 to 7.71, I2 = 0%, p < 0.001), reduced left ventricular end-systolic volume (MD: -23.47 ml, 95% CI: -37.18 to -9.13, p < 0.001), and reduced left ventricular end-diastolic volume (MD: -24.02 ml, 95% CI: -37.01 to -11.03, p = 0.02).
Conclusion: Evidence from current studies suggests that leadless endocardial LV pacing resynchronization is effective for HF patients who failed conventional CRT or needed a device upgrade, and it may be an interesting rescue therapy.
Keywords: CRT; WiSE system; endocardial pacing; heart failure; leadless cardiac pacing.
Copyright © 2022 Cang, Liu, Zhu, Liu, Shen, Miao, Zhou and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Leadless left ventricular endocardial pacing in nonresponders to conventional cardiac resynchronization therapy.Pacing Clin Electrophysiol. 2020 Sep;43(9):966-973. doi: 10.1111/pace.13926. Epub 2020 May 9. Pacing Clin Electrophysiol. 2020. PMID: 32330307
-
Feasibility, safety, and short-term outcome of leadless ultrasound-based endocardial left ventricular resynchronization in heart failure patients: results of the wireless stimulation endocardially for CRT (WiSE-CRT) study.Europace. 2014 May;16(5):681-8. doi: 10.1093/europace/eut435. Epub 2014 Feb 4. Europace. 2014. PMID: 24497573
-
Efficacy of Leadless Ultrasound-Based Left Ventricular Endocardial Pacing for Cardiac Resynchronization Therapy: A Meta-Analysis.Cardiol Rev. 2025 Mar 26. doi: 10.1097/CRD.0000000000000897. Online ahead of print. Cardiol Rev. 2025. PMID: 40135909
-
Leadless left ventricular endocardial pacing for cardiac resynchronization therapy: A systematic review and meta-analysis.Heart Rhythm. 2022 Jul;19(7):1176-1183. doi: 10.1016/j.hrthm.2022.02.018. Epub 2022 Feb 18. Heart Rhythm. 2022. PMID: 35189383
-
The therapeutic effects of upgrade to cardiac resynchronization therapy in pacing-induced cardiomyopathy or chronic right ventricular pacing patients: a meta-analysis.Heart Fail Rev. 2022 Mar;27(2):507-516. doi: 10.1007/s10741-021-10091-z. Epub 2021 Feb 27. Heart Fail Rev. 2022. PMID: 33638772 Review.
Cited by
-
Current Advance, Challenges and Future Perspectives of Conduction System Pacing.Rev Cardiovasc Med. 2024 Dec 16;25(12):438. doi: 10.31083/j.rcm2512438. eCollection 2024 Dec. Rev Cardiovasc Med. 2024. PMID: 39742235 Free PMC article. Review.
References
-
- Seifert M, Schau T, Moeller V, Neuss M, Meyhoefer J, Butter C. Influence of pacing configurations, body mass index, and position of coronary sinus lead on frequency of phrenic nerve stimulation and pacing thresholds under cardiac resynchronization therapy. Europace. (2010) 12:961–7. 10.1093/europace/euq119 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous