

Primary vs. Secondary Heart Failure Diagnosis: Differences in Clinical Outcomes, Healthcare Resource Utilization and Cost
- PMID: 35369321
- PMCID: PMC8967997
- DOI: 10.3389/fcvm.2022.818525
Primary vs. Secondary Heart Failure Diagnosis: Differences in Clinical Outcomes, Healthcare Resource Utilization and Cost
Abstract
Background: There is scarce information on patients with secondary heart failure diagnosis (sHF). We aimed to compare the characteristics, burden, and outcomes of sHF with those with primary HF diagnosis (pHF).
Methods: Retrospective, observational study on patients ≥18 years with emergency department (ED) visits during 2018 with pHF and sHF in ED or hospital (ICD-10-CM) diagnostic codes. Baseline characteristics, 30-day and 1-year mortality, readmission and re-ED visit rates, and costs were compared between sHF and pHF.
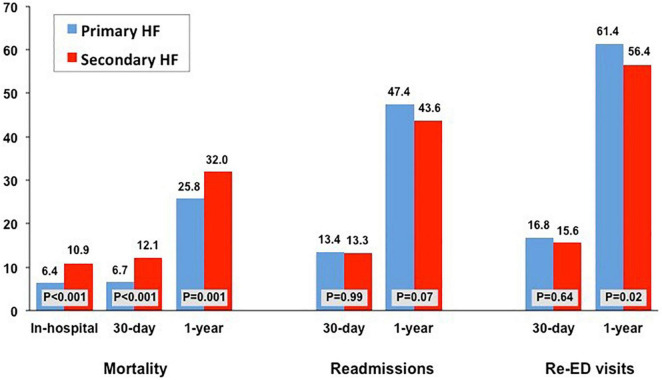
Results: Out of the 797 patients discharged home from the ED, 45.5% had sHF, and these presented lower 1-year hospitalization, re-ED visit rates, and costs. In contrast, out of the 2,286 hospitalized patients, 55% had sHF and 45% pHF. Hospitalized sHF patients had significantly (p < 0.01) greater comorbidity, lower use of recommended HF therapies, longer length of stay (10.8 ± 10.1 vs. 9.7 ± 7.9 days), and higher in-hospital and 1-year mortality (32 vs. 25.8%) with no significant differences in readmission rates and lower 1-year re-ED visit rate. Hospitalized sHF patients had higher total costs (€12,262,422 vs. €9,144,952, p < 0.001), mean cost per patient-year (€9,755 ± 13,395 vs. €8,887 ± 12,059), and average daily cost per patient.
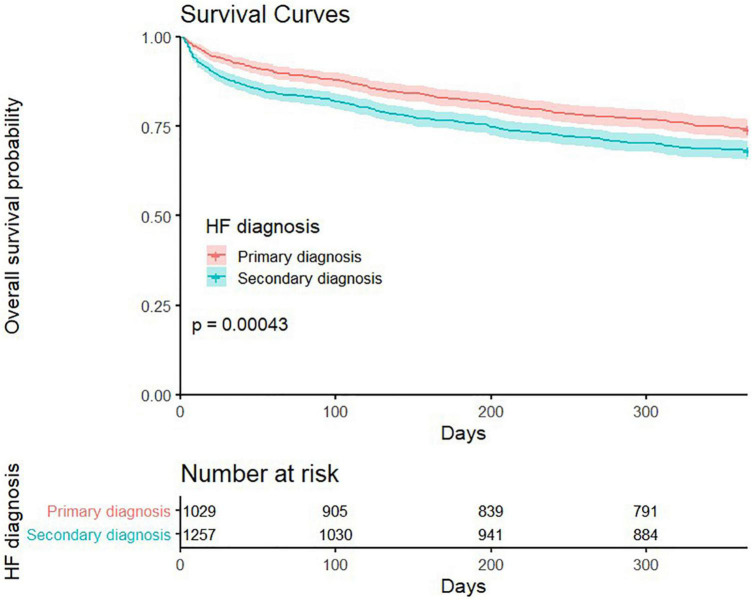
Conclusion: Hospitalized sHF patients have a worse initial prognosis, greater use of healthcare resources, and higher costs.
Keywords: cost; heart failiure; mortality; outcome; resource utilization; secondary diagnosis.
Copyright © 2022 Bueno, Goñi, Salguero-Bodes, Palacios, Vicent, Moreno, Rosillo, Varela, Capel, Delgado, Arribas, del Oro, Ortega and Bernal.
Conflict of interest statement
HB receives research funding from the Instituto de Salud Carlos III, Spain (PIE16/00021 and PI17/01799), Sociedad Española de Cardiología, Astra-Zeneca, Bayer, PhaseBio and Novartis; has received consulting fees from Astra-Zeneca, Novartis; and speaking fees from Novartis and MEDSCAPE-the heart.og. BP, LVa, and MC are AstraZeneca Spain employees. JB reports grant from AstraZeneca, during the conduct of the study. FA reports personal fees from Daiichi Sankyo, personal fees from Impulse Dynamics, personal fees from Medtronic, personal fees from Boston Scientific, personal fees from Bayer, personal fees from Bristol Myers Squibb, personal fees from Arrhythmia Network Technology SL/BAROSTIM, personal fees from Abbott, outside the submitted work. JD reports personal fees from Novartis, personal fees from Astra Zeneca, personal fees from Boehringer, outside the submitted work. RS-B reports other from Boston Scientific, non-financial support from Medtronic, personal fees and other from Daichii Sankyo, and other from Abbott, outside the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Méndez-Bailón M, Jiménez-García R, Hernández-Barrera V, Comín-Colet J, Esteban-Hernández J, de Miguel-Díez J, et al. Significant and constant increase in hospitalization due to heart failure in Spain over 15 year period. Eur J Intern Med. (2019) 64:48–56. - PubMed
-
- Bueno H, Bernal JL, Jiménez-Jiménez V, Martín-Sánchez FJ, Rossello X, Moreno G, et al. The clinical outcomes, healthcare resource utilization, and related costs (COHERENT) model. application in heart failure patients. Rev Esp Cardiol (Engl Ed). (2021). 10.1016/j.rec.2021.08.009 [Epub ahead of print]. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous