

Trainee-led Engagement of the Care Team Improves Application of an Institutional Blood Culture Clinical Decision Algorithm to Pediatric Oncology Inpatients: A Single-institution Quality Improvement Project
- PMID: 35369412
- PMCID: PMC8970086
- DOI: 10.1097/pq9.0000000000000545
Trainee-led Engagement of the Care Team Improves Application of an Institutional Blood Culture Clinical Decision Algorithm to Pediatric Oncology Inpatients: A Single-institution Quality Improvement Project
Abstract
Meaningful engagement in quality improvement (QI) projects by trainees is often challenging. A fellow-led QI project aimed to improve adherence to a blood culture clinical decision algorithm and reduce unnecessary cultures in pediatric oncology inpatients.
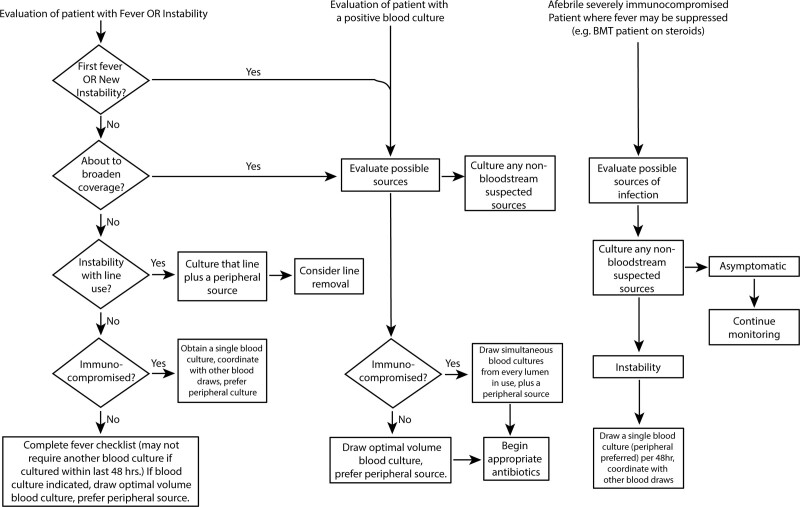
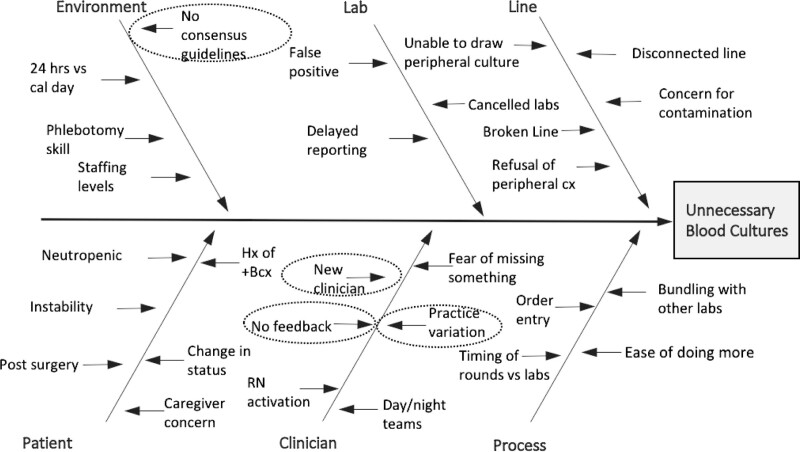
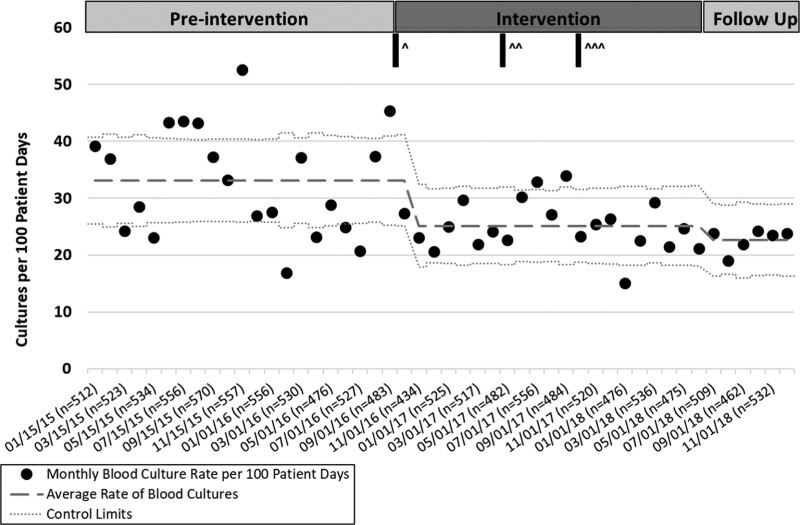
Methods: We visualized preintervention rates of blood cultures drawn on pediatric oncology inpatients using a control chart. Following the introduction of the algorithm to our division, an Ishikawa fishbone diagram of cause-and-effect identified two areas for improvement: prescriber education on the algorithm and targeted feedback on its use. We developed two interventions to support algorithm awareness and use: (1) bundled educational interventions and (2) targeted chart review and feedback. Fellows reviewed >750 blood culture episodes and adjudicated each as "adherent" or "nonadherent" to the algorithm. In addition, fellows provided direct feedback to prescribers regarding nonadherent episodes and discussed strategies for algorithm adherence.
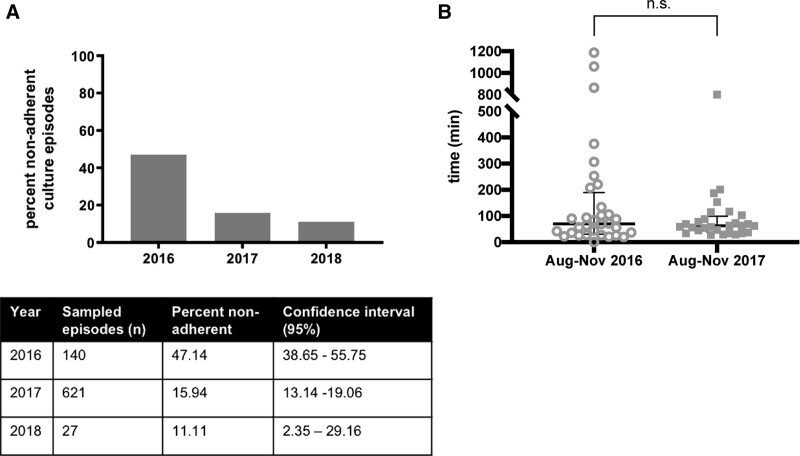
Results: Blood culture rates in preintervention, intervention, and follow-up periods were 33.35, 25.24, and 22.67 cultures/100 patient-days, respectively. The proportion of nonadherent culture episodes decreased from 47.14% to 11.11%. The use of the algorithm did not prolong the time to cultures drawn on patients with new fever. Seventy-five percent of fellows provided feedback to inpatient teams on algorithm use. Following this project, trainees reported feeling more qualified to apply QI principles to patient care.
Conclusions: Implementation of a clinical decision algorithm reduced the rate of cultures drawn on pediatric oncology inpatients. Fellow-led education of the care team decreased the proportion of nonadherent culture episodes and provided active engagement in QI.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Figures
References
-
- Accreditation Council for Graduate Medical Education (ACGME). National Report of Findings: Executive Summary. 2016. Clinical Learning Environment Review. https://www.acgme.org/Portals/0/PDFs/CLER/ACGME-CLER-ExecutiveSummary.pdf
-
- Kouo T, Kleinman K, Fujii-Rios H, et al. . A resident-led QI initiative to improve pediatric emergency department boarding times. Pediatrics. 2020;145:e20191477. - PubMed
-
- Patow CA, Karpovich K, Riesenberg LA, et al. . Residents’ engagement in quality improvement: a systematic review of the literature. Acad Med. 2009;84:1757–1764. - PubMed
-
- Woods-Hill CZ, Fackler J, Nelson McMillan K, et al. . Association of a clinical practice guideline with blood culture use in critically ill children. JAMA Pediatr. 2017;171:157–164. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources