

Patency Outcomes of Arteriovenous Fistulas and Grafts for Hemodialysis Access: A Trade-Off between Nonmaturation and Long-Term Complications
- PMID: 35369548
- PMCID: PMC8815607
- DOI: 10.34067/KID.0000462020
Patency Outcomes of Arteriovenous Fistulas and Grafts for Hemodialysis Access: A Trade-Off between Nonmaturation and Long-Term Complications
Abstract
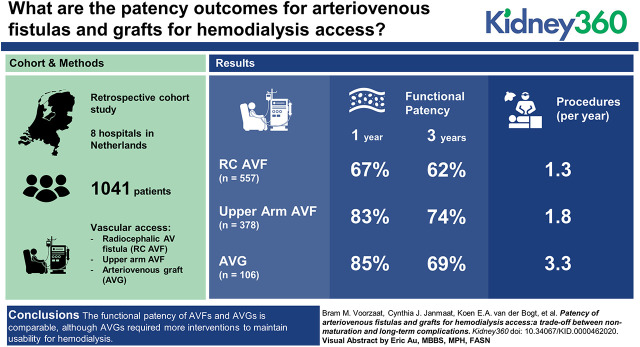
Background: Arteriovenous fistulas (AVFs) for hemodialysis (HD) are often associated with better outcomes than arteriovenous grafts (AVGs). We aimed to investigate vascular access (VA) outcomes and assessed if AVF nonmaturation outweighs long-term complications of AVGs.
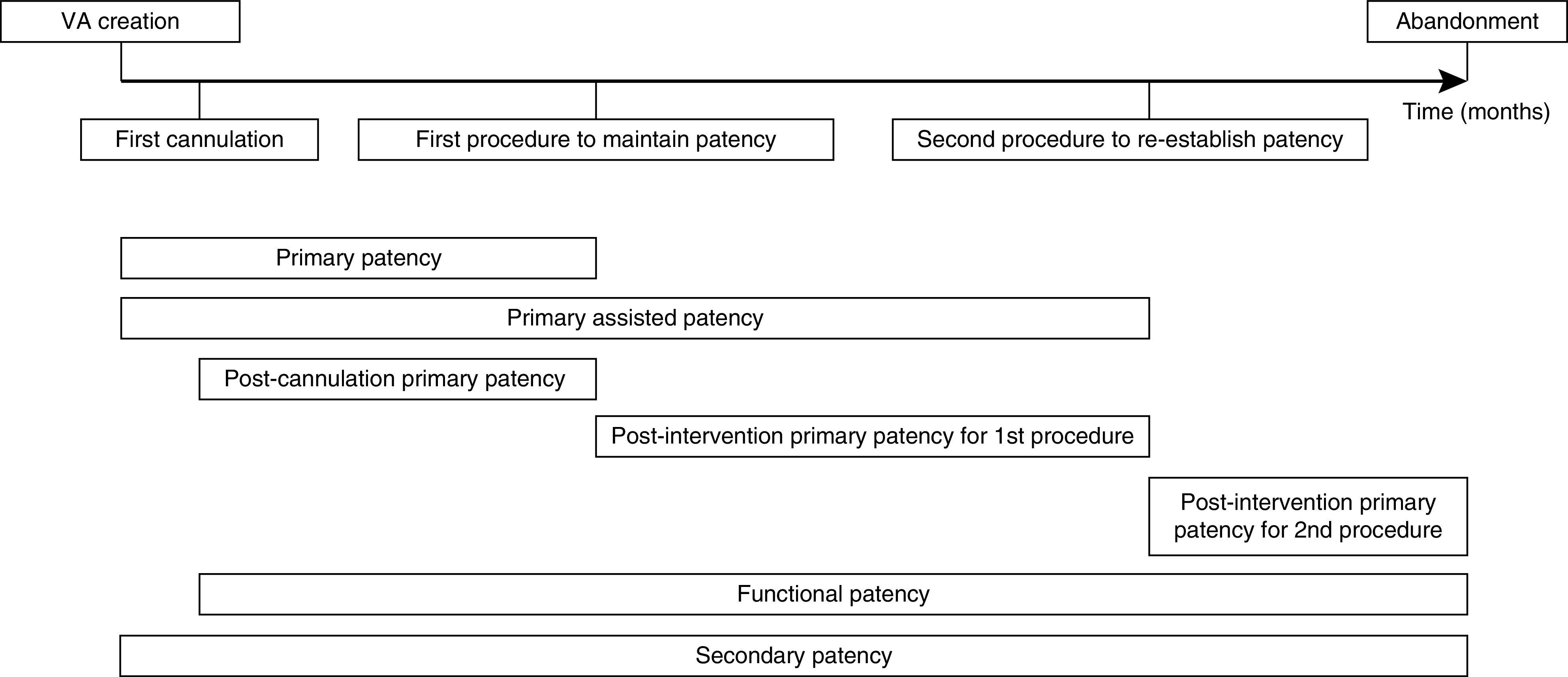
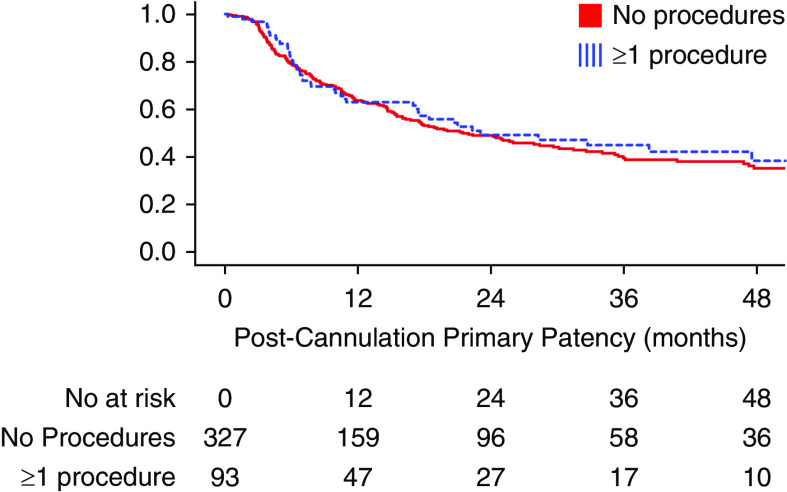
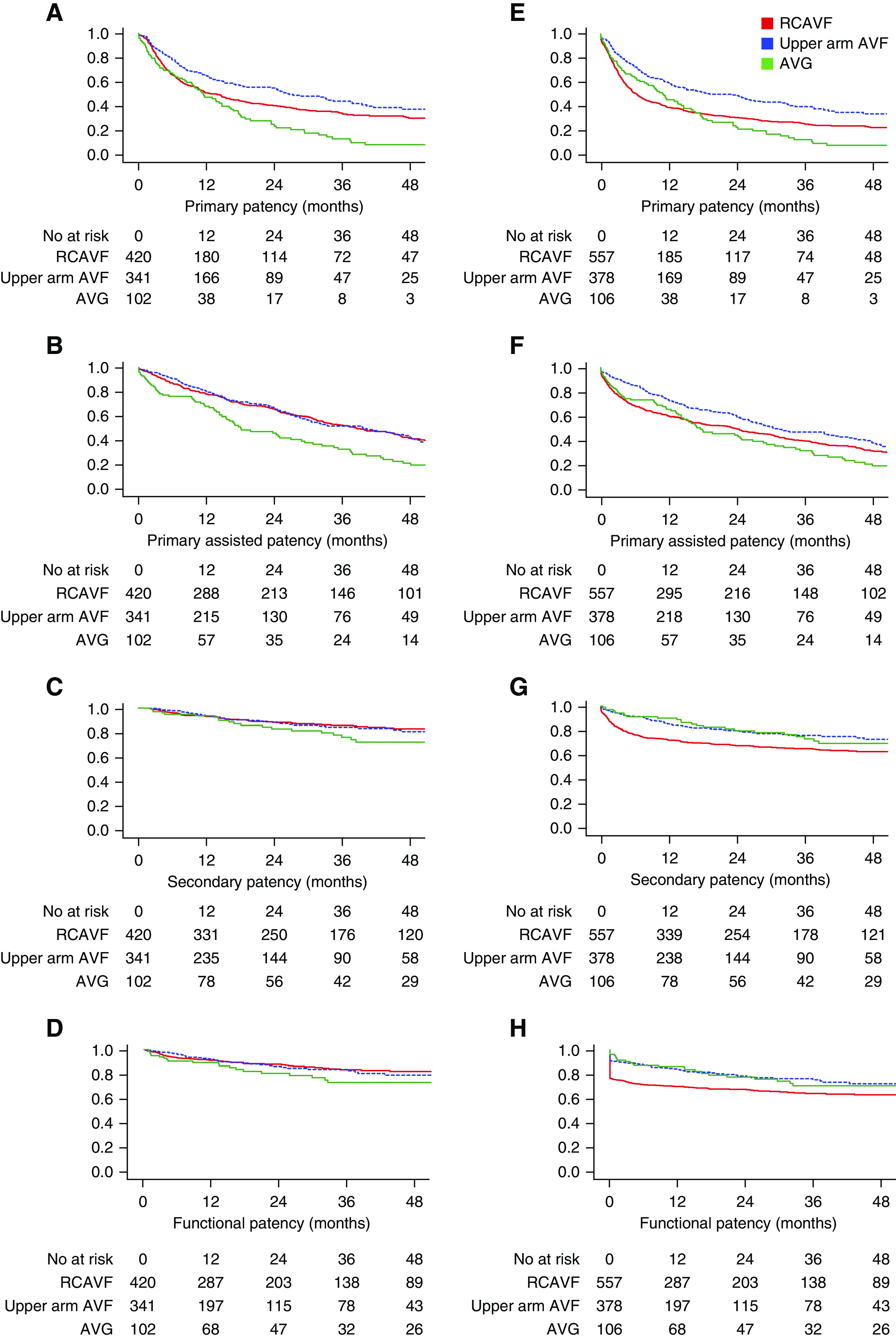
Methods: In this multicenter, retrospective cohort study in The Netherlands, 1- and 3-year primary, primary assisted, secondary, and functional patency rates were calculated, and the incidence of adverse events and procedures was assessed. Functional patency of RCAVFs, upper arm AVFs, and AVGs was compared using Cox analyses.
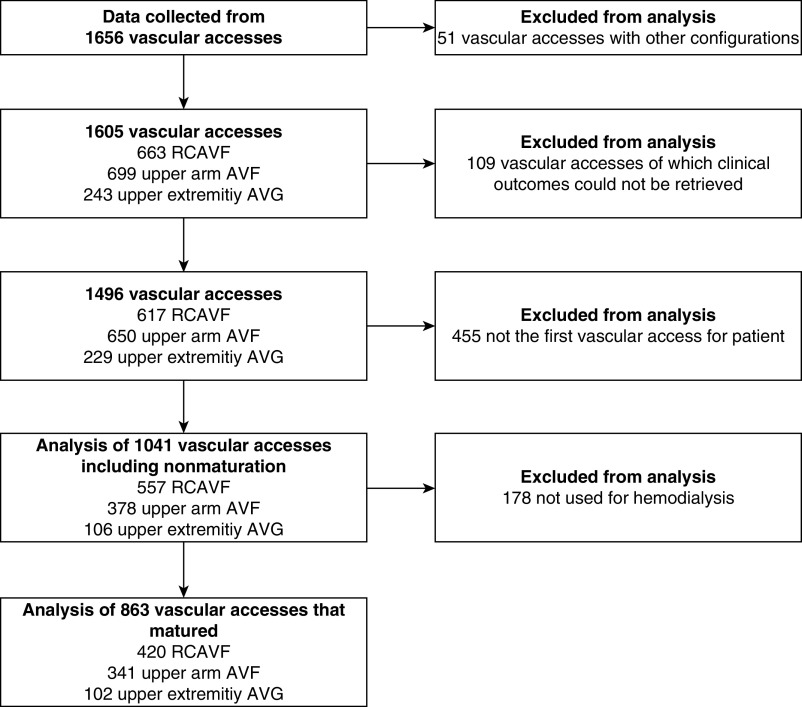
Results: In total, 1041 patients who received their first VA were included, of whom 863 had VAs that successfully matured. These patients were analyzed with a median follow-up of 25 months. The 1-year functional patency rates were 67%±2.0% for RCAVFs, 83%±2.0% for upper arm AVFs, and 85%±3.5% for AVGs. Three-year functional patency rates were 62%±2.0% for RCAVFs, 74%±2.0% for upper arm AVFs, and 69%±5% for AVGs. AVGs required more procedures per year (3.3 per year) of functional patency when compared with upper arm AVFs (1.8 per year).
Conclusions: The functional patency of AVFs and AVGs is comparable, although AVGs required more interventions to maintain usability for HD. The choice of VA is a trade-off between short-term advantages, favoring AVGs, and long-term advantages, favoring AVFs. Which VA is most appropriate depends on the patient's prognosis and preferences.
Keywords: arteriovenous fistula; arteriovenous graft; dialysis; patency; vascular access.
Copyright © 2020 by the American Society of Nephrology.
Conflict of interest statement
All authors have nothing to disclose.
Figures
References
-
- Tordoir J, Canaud B, Haage P, Konner K, Basci A, Fouque D, Kooman J, Martin-Malo A, Pedrini L, Pizzarelli F, Tattersall J, Vennegoor M, Wanner C, Wee Pt, et al. R: EBPG on vascular access. Nephrol Dial Transplant 22[Suppl 2]: ii88–ii117, 2007 - PubMed
-
- Schmidli J, Widmer MK, Basile C, de Donato G, Gallieni M, Gibbons CP, Haage P, Hamilton G, Hedin U, Kamper L, Lazarides MK, Lindsey B, Mestres G, Pegoraro M, Roy J, Setacci C, Shemesh D, Tordoir JHM, van Loon M, Kolh P, de Borst GJ, Chakfe N, Debus S, Hinchliffe R, Kakkos S, Koncar I, Lindholt J, Naylor R, Vega de Ceniga M, Vermassen F, Verzini F, Mohaupt M, Ricco JB, Roca-Tey R; ESVS Guidelines Committee; ESVS Guidelines Reviewers : Editor’s choice—vascular access: 2018 Clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 55: 757–818, 2018 - PubMed
-
- Rothuizen TC, Wong C, Quax PHA, van Zonneveld AJ, Rabelink TJ, Rotmans JI: Arteriovenous access failure: More than just intimal hyperplasia? Nephrol Dial Transplant 28: 1085–1092, 2013 - PubMed
-
- Pisoni RL, Young EW, Dykstra DM, Greenwood RN, Hecking E, Gillespie B, Wolfe RA, Goodkin DA, Held PJ: Vascular access use in Europe and the United States: Results from the DOPPS. Kidney Int 61: 305–316, 2002 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
