

Use of Ultrasound to Assess Hemodynamics in Acutely Ill Patients
- PMID: 35369668
- PMCID: PMC8676393
- DOI: 10.34067/KID.0002322021
Use of Ultrasound to Assess Hemodynamics in Acutely Ill Patients
Abstract
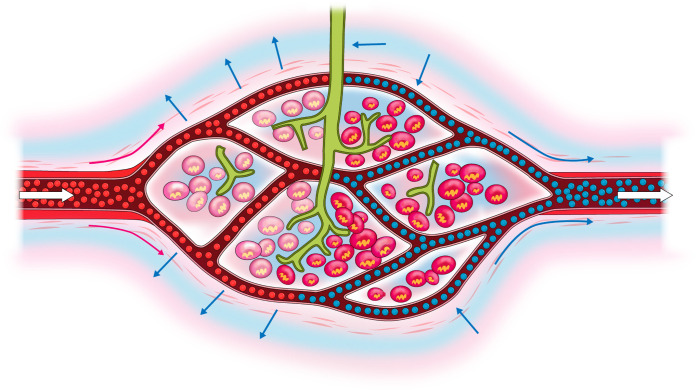
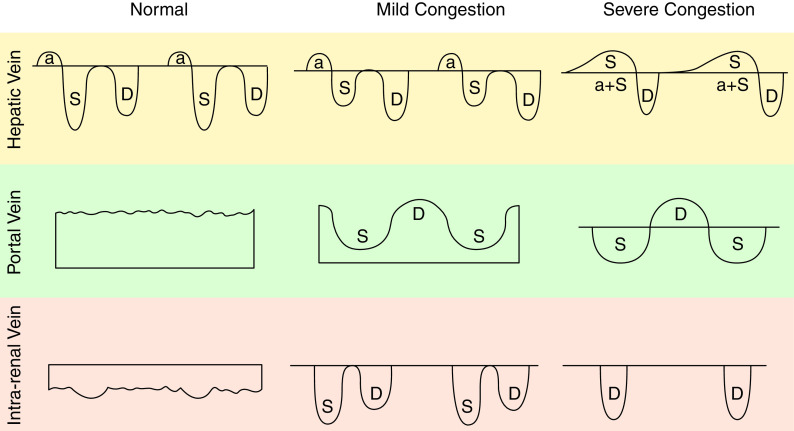
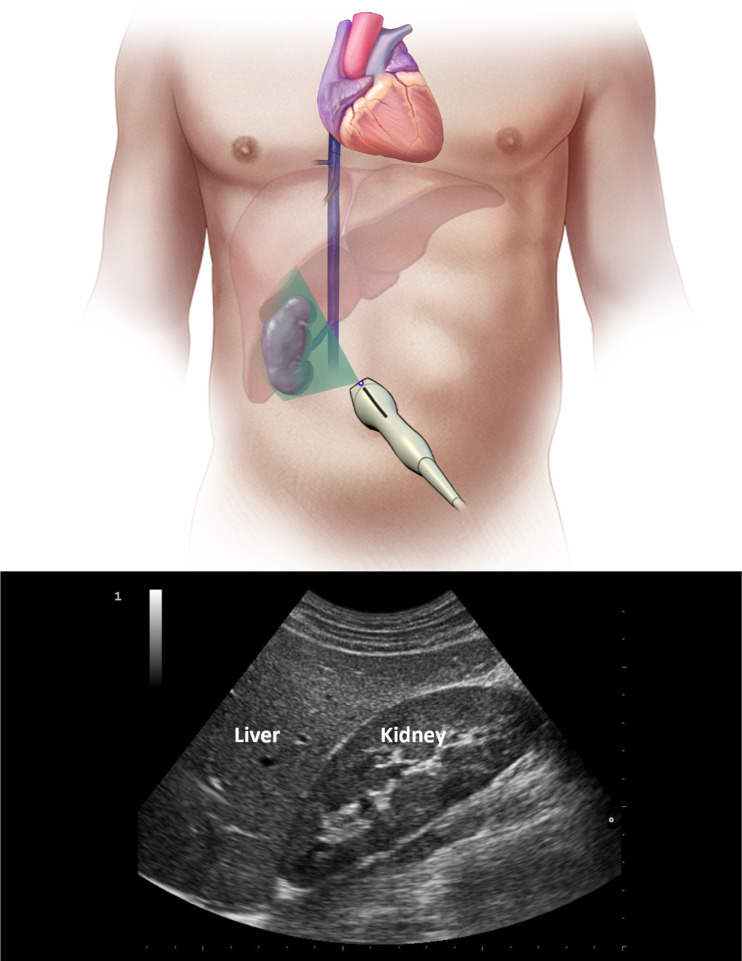
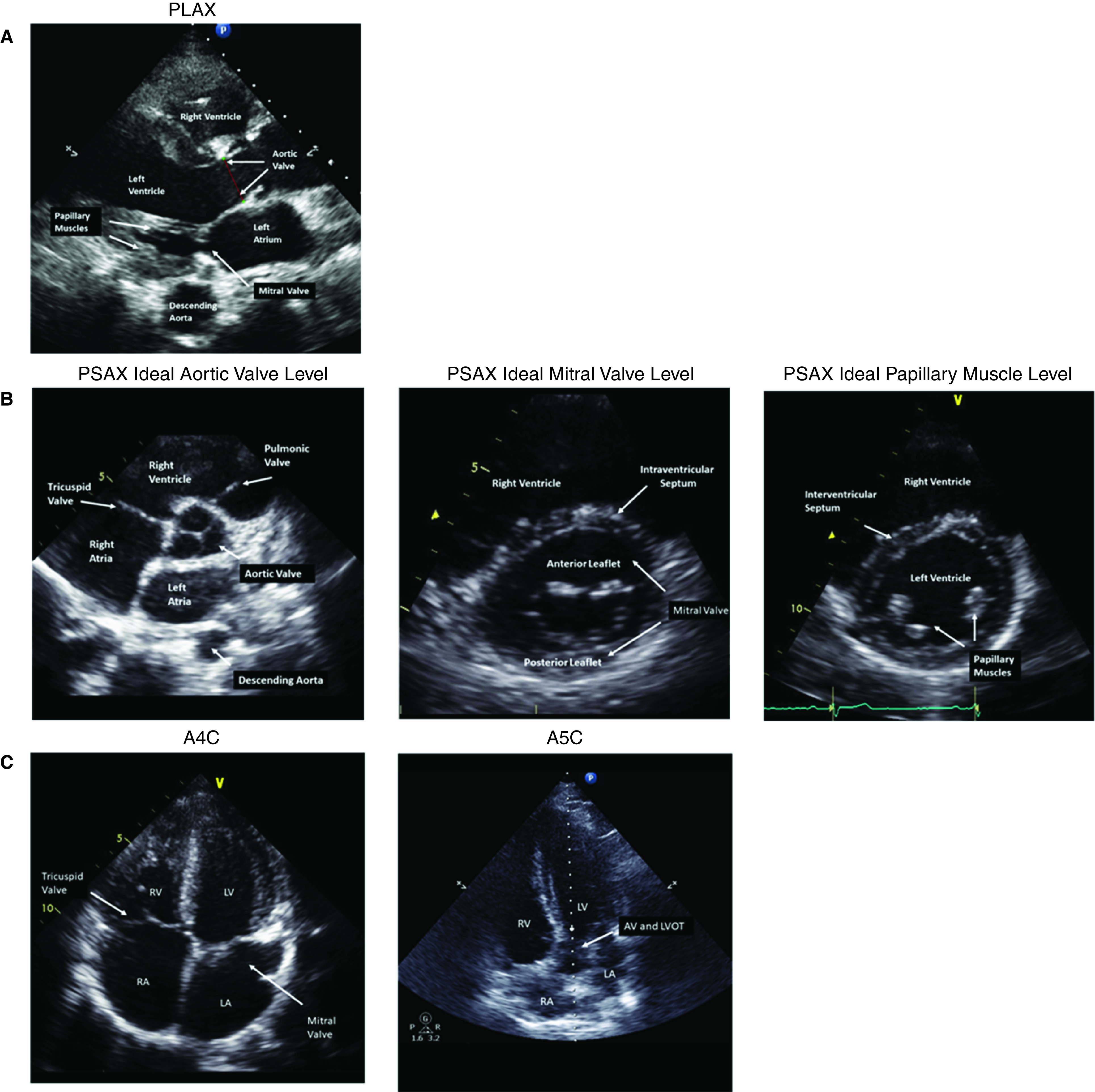
Early diagnosis of AKI and preventive measures can likely decrease the severity of the injury and improve patient outcomes. Current hemodynamic monitoring variables, including BP, heart and respiratory rates, temperature, and oxygenation status, have been used to identify patients at high risk for AKI. Despite the widespread use of such variables, their ability to accurately and timely detect patients who are high risk has been questioned. Therefore, there is a critical need to develop and validate tools that can measure new and more kidney-specific hemodynamic and laboratory variables, potentially assisting with AKI risk stratification, implementing appropriate and timely preventive measures, and hopefully improved outcomes. The new ultrasonography techniques provide novel insights into kidney hemodynamics and potential management and/or therapeutic targets. Contrast-enhanced ultrasonography; Doppler flow patterns of hepatic veins, portal vein, and intrakidney veins; and ultrasound elastography are among approaches that may provide such information, particularly related to vascular changes in AKI, venous volume excess or congestion, and fluid tolerance. This review summarizes the current state of these techniques and their relevance to kidney hemodynamic management.
Keywords: AKI; IVF; POCU; acute kidney injury; acute kidney injury and ICU nephrology; hemodynamics; intravenous fluids; kidney congestion; ultrasound; volume overload; volume tolerance.
Copyright © 2021 by the American Society of Nephrology.
Conflict of interest statement
K.B. Kashani reports having consultancy agreements with AM Pharma; serving as a scientific advisor for, or member of, GE, La Jolla Inc., and MediBeacon Inc.; and receiving research funding from La Jolla Inc. All remaining authors have nothing to disclose.
Figures




References
-
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, Kumar A, Sevransky JE, Sprung CL, Nunnally ME, Rochwerg B, Rubenfeld GD, Angus DC, Annane D, Beale RJ, Bellinghan GJ, Bernard GR, Chiche JD, Coopersmith C, De Backer DP, French CJ, Fujishima S, Gerlach H, Hidalgo JL, Hollenberg SM, Jones AE, Karnad DR, Kleinpell RM, Koh Y, Lisboa TC, Machado FR, Marini JJ, Marshall JC, Mazuski JE, McIntyre LA, McLean AS, Mehta S, Moreno RP, Myburgh J, Navalesi P, Nishida O, Osborn TM, Perner A, Plunkett CM, Ranieri M, Schorr CA, Seckel MA, Seymour CW, Shieh L, Shukri KA, Simpson SQ, Singer M, Thompson BT, Townsend SR, Van der Poll T, Vincent JL, Wiersinga WJ, Zimmerman JL, Dellinger RP: Surviving Sepsis Campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med 43: 304–377, 2017. 10.1007/s00134-017-4683-6 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
