

Myelitis: A Common Complication of Tuberculous Meningitis Predicting Poor Outcome
- PMID: 35370906
- PMCID: PMC8965833
- DOI: 10.3389/fneur.2022.830029
Myelitis: A Common Complication of Tuberculous Meningitis Predicting Poor Outcome
Abstract
Background: Myelitis is an important complication in patients with tuberculous meningitis (TBM). However, a paucity of publications exists on the spectrum of neurological and MRI findings of TBM-related myelitis. The risk factors and prognosis of myelitis in patients with TBM are not fully understood. Therefore, this study aims to identify the risk factors, clinicoradiological features, and prognostic impact of myelitis for patients with TBM.
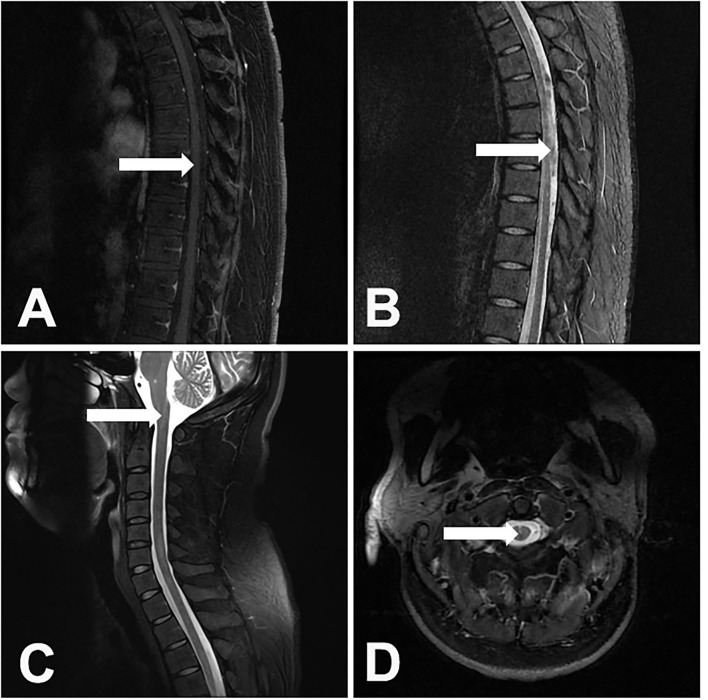
Methods: We conducted a retrospective study in our institution. Patients with TBM who were consecutively admitted during the period of August 2015 to December 2019 were included. We reviewed the demographic characteristics, clinical, laboratory and MRI findings, and clinical outcomes of all of the included patients. The diagnosis of myelitis was identified by a hyperintensity on T2-weighted images that were associated with cord edema, enlargement, and marginal or no enhancement on contrast-enhanced images.
Results: A total of 114 patients were included. Myelitis occurred in 19 (16.7%) patients, five of whom paradoxically developed myelitis. The common clinical signs of myelitis were paraparesis (738.9%), quadriparesis (844.4%), urinary retention or constipation (1,477.8%), and paresthesias in the lower limbs (1,052.6%). In the MRI findings, the hyperintensities on T2-weighted images involved more than 3 spinal cord segments. Myelitis was often combined with other forms of spinal cord injury, including 10 patients (52.6%) with spinal meningeal enhancement, 7 patients (36.8%) with enlargement of the central canal of the spinal cord, 6 patients (31.6%) with tuberculoma, and 4 patients (21.1%) with arachnoiditis and 1 patient (5.3%) with cerebrospinal fluid (CSF) loculations. None of the 5 patients with paradoxical myelitis were complicated with spinal meningeal enhancement and arachnoiditis, while 4 patients were complicated with enlargements of the central canal of the spinal cord. In multivariable analysis, a grade III disease severity on admission [p = 0.003, odds ratio (OR) = 8.131, 95% CI: 2.080-31.779] and high CSF protein (p = 0.033, OR = 1.698, 95% CI: 1.043-2.763) were independent risk factors for myelitis. After the 6 months follow-up, myelitis (p = 0.030, OR = 13.297, 95% CI: 1.283-137.812) and disturbance of consciousness (p = 0.042, OR = 12.625, 95% CI: 1.092-145.903) were independent risk factors for poor outcomes.
Conclusion: Myelitis was a common complication of TBM and independently predicted a poor outcome. A grade III disease severity and high CSF protein on admission were independent risk factors for myelitis. Paradoxical myelitis was rarely complicated with spinal meningeal enhancements and arachnoiditis, indicating that the immune reaction may play a dominant role.
Keywords: immune reaction; myelitis; paradoxical reaction; prognosis; tuberculous meningitis.
Copyright © 2022 Jiang, Xu, Guo, Liu, Lin, Suo, Jiang, Liu and Lu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Spinal cord and spinal nerve root involvement (myeloradiculopathy) in tuberculous meningitis.Medicine (Baltimore). 2015 Jan;94(3):e404. doi: 10.1097/MD.0000000000000404. Medicine (Baltimore). 2015. PMID: 25621686 Free PMC article.
-
Seropositive Neuromyelitis Optica in a Case of Undiagnosed Ankylosing Spondylitis: A Neuro-Rheumatological Conundrum.Qatar Med J. 2022 Jul 7;2022(3):29. doi: 10.5339/qmj.2022.29. eCollection 2022. Qatar Med J. 2022. PMID: 35864917 Free PMC article.
-
Tuberculous myelitis: a prospective follow-up study.Neurol Sci. 2022 Sep;43(9):5615-5624. doi: 10.1007/s10072-022-06221-6. Epub 2022 Jun 23. Neurol Sci. 2022. PMID: 35739331 Free PMC article.
-
Spinal cord involvement in tuberculous meningitis.Spinal Cord. 2015 Sep;53(9):649-57. doi: 10.1038/sc.2015.58. Epub 2015 Apr 21. Spinal Cord. 2015. PMID: 25896347 Review.
-
Tuberculous radiculomyelitis complicating tuberculous meningitis: case report and review.Clin Infect Dis. 2000 Jun;30(6):915-21. doi: 10.1086/313821. Epub 2000 Jun 14. Clin Infect Dis. 2000. PMID: 10854362 Review.
Cited by
-
A case report of long-segment tuberculous myelitis with concomitant tuberculous meningitis.AME Case Rep. 2025 Jun 6;9:76. doi: 10.21037/acr-24-211. eCollection 2025. AME Case Rep. 2025. PMID: 40761219 Free PMC article.
-
Isolated Tuberculous Transverse Myelitis Without Meningitis Among Patients With AIDS: A Case Report.Cureus. 2023 Dec 17;15(12):e50650. doi: 10.7759/cureus.50650. eCollection 2023 Dec. Cureus. 2023. PMID: 38229805 Free PMC article.
-
Clinical Approach to Myelopathy Diagnosis.Continuum (Minneap Minn). 2024 Feb 1;30(1):14-52. doi: 10.1212/CON.0000000000001390. Continuum (Minneap Minn). 2024. PMID: 38330471 Free PMC article.
-
Central Nervous System Tuberculosis in Immunocompromised Patients: A Case Report Emphasizing Immune Status and Early Recognition and Treatment.Cureus. 2024 Jan 22;16(1):e52715. doi: 10.7759/cureus.52715. eCollection 2024 Jan. Cureus. 2024. PMID: 38260110 Free PMC article.
-
Acute ischemic stroke in tuberculous meningitis.Front Public Health. 2024 Mar 21;12:1362465. doi: 10.3389/fpubh.2024.1362465. eCollection 2024. Front Public Health. 2024. PMID: 38577289 Free PMC article.
References
-
- Moghtaderi A, Alavi Naini R. Tuberculous radiculomyelitis: review and presentation of five patients. Int J Tuberc Lung Dis. (2003) 7:1186–90. - PubMed
LinkOut - more resources
Full Text Sources