

Comparative Cardiovascular Outcomes of SGLT2 Inhibitors in Type 2 Diabetes Mellitus: A Network Meta-Analysis of Randomized Controlled Trials
- PMID: 35370961
- PMCID: PMC8967154
- DOI: 10.3389/fendo.2022.802992
Comparative Cardiovascular Outcomes of SGLT2 Inhibitors in Type 2 Diabetes Mellitus: A Network Meta-Analysis of Randomized Controlled Trials
Abstract
Background: A network meta-analysis of randomized controlled trials (RCTs) was conducted to explore the cardiovascular outcomes of all the kind and dosages of sodium-glucose cotransport-2 (SGLT2) inhibitors in type 2 diabetes mellitus (T2DM) patients.
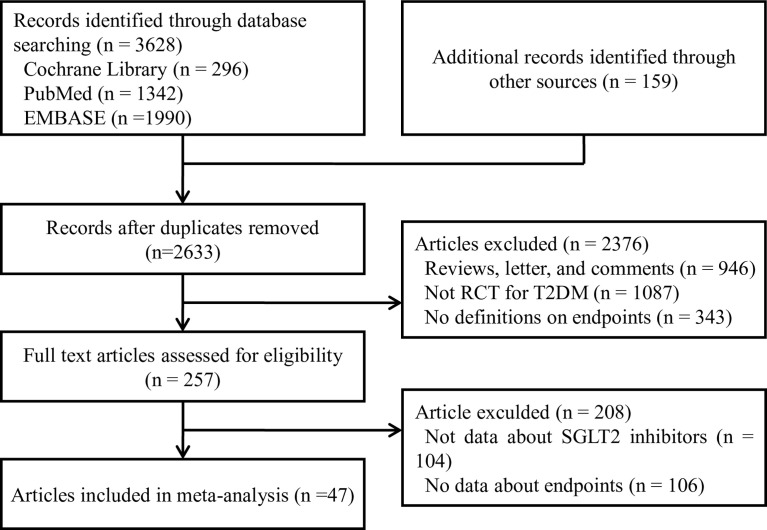
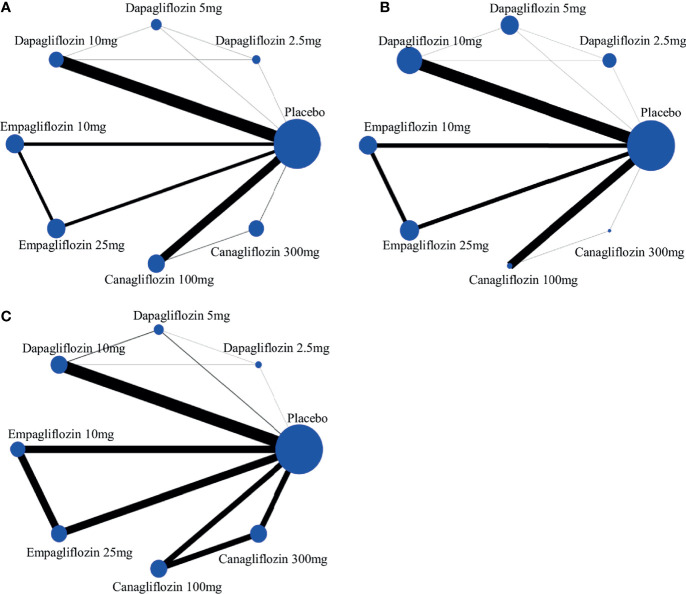
Method and result: The Cochrane Library, PubMed, and Embase databases were systematically searched for studies to compare the therapeutic effects of different SGLT2 inhibitors in T2DM patients. The effect measurements estimate chosen were odds ratios (ORs) and their corresponding 95% confidence interval (CI). Forty-seven RCTs involving a total of 70574 participants were eligible for direct and indirect comparisons. In direct comparison, treatment with dapagliflozin 5mg showed significantly lower risk of all-cause mortality compared with treatment with dapagliflozin 2.5mg (OR 0.09, 95% CI 0.01-0.70). According to NMA, interestingly, empagliflozin 10mg/25mg, and canagliflozin 100mg was associated with significantly lower risks of all-cause mortality compared with placebo (OR of 0.70, 95% CI 0.58-0.85; 0.69, 95% CI 0.57-0.84; and 0.83, 95% CI 0.73-0.95, respectively). Compared with placebo, dapagliflozin 10mg, empagliflozin 10mg and 25mg displayed the lower risks for cardiovascular events (OR 0.78, 95% CI 0.44-1.00; OR 0.47, 95% CI 0.22-0.93; and 0.43, 95% CI 0.24-0.74, respectively) by direct comparison. Moreover, canagliflozin 100/300mg showed significantly higher risks of cardiovascular events compared with empagliflozin 10mg (OR of 4.83, 95% CI 1.14-20.46 and 5.31, 95% CI 1.26-22.34, respectively) and empagliflozin 25mg (4.23, 95% CI 1.13-15.83 and 4.65, 95% CI 1.25-17.27, respectively) according to NMA. There were non-significant differences among all interventions in volume depletion in traditional pairwise meta-analysis. While in NMA, canagliflozin 100/300mg were associated with significantly increased risks of volume depletion compared with placebo (OR of 1.47, 95% CI 1.08-1.99 and 2.19, 95% CI 1.66-2.90, respectively).
Conclusion: In the limitations of the NMA, this study showed that empagliflozin might be better than other SGLT2 inhibitors with low risks of all-cause mortality and cardiovascular events in patients with T2DM suggesting the need for ad hoc RCTs.
Keywords: SGLT2 inhibitors; cardiovascular events; empagliflozin; meta-analysis; type 2 diabetes mellitus.
Copyright © 2022 Jiang, Yang, Fu, Sun, Shen and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Emerging Risk Factors C, Sarwar N, Gao P, Seshasai SR, Gobin R, Kaptoge S, et al. . Diabetes Mellitus, Fasting Blood Glucose Concentration, and Risk of Vascular Disease: A Collaborative Meta-Analysis of 102 Prospective Studies. Lancet (2010) 375(9733):2215–22. doi: 10.1016/S0140-6736(10)60484-9 - DOI - PMC - PubMed
-
- Lexis CP, van der Horst IC, Lipsic E, Wieringa WG, de Boer RA, van den Heuvel AF, et al. . Effect of Metformin on Left Ventricular Function After Acute Myocardial Infarction in Patients Without Diabetes: The GIPS-III Randomized Clinical Trial. Jama (2014) 311(15):1526–35. doi: 10.1001/jama.2014.3315 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical