

Definition of the Immune Parameters Related to COVID-19 Severity
- PMID: 35371011
- PMCID: PMC8971756
- DOI: 10.3389/fimmu.2022.850846
Definition of the Immune Parameters Related to COVID-19 Severity
Erratum in
-
Corrigendum: Definition of the immune parameters related to COVID-19 severity.Front Immunol. 2023 May 24;14:1219179. doi: 10.3389/fimmu.2023.1219179. eCollection 2023. Front Immunol. 2023. PMID: 37292212 Free PMC article.
Abstract
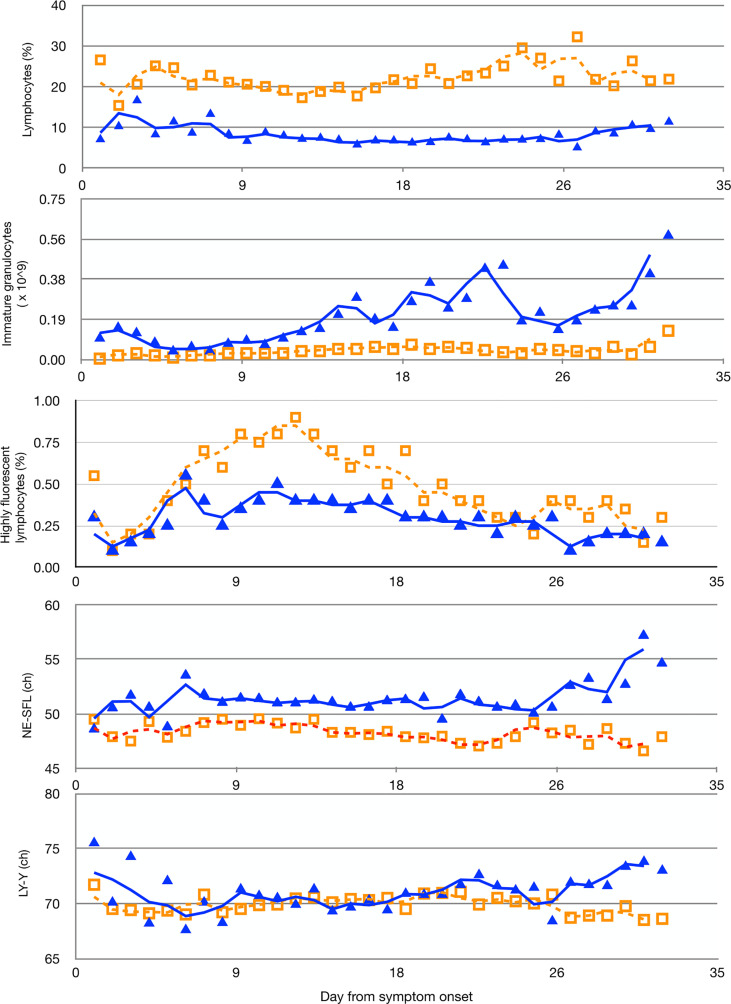
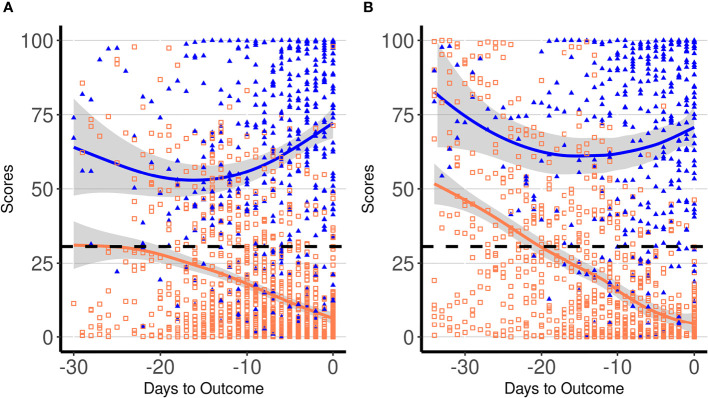
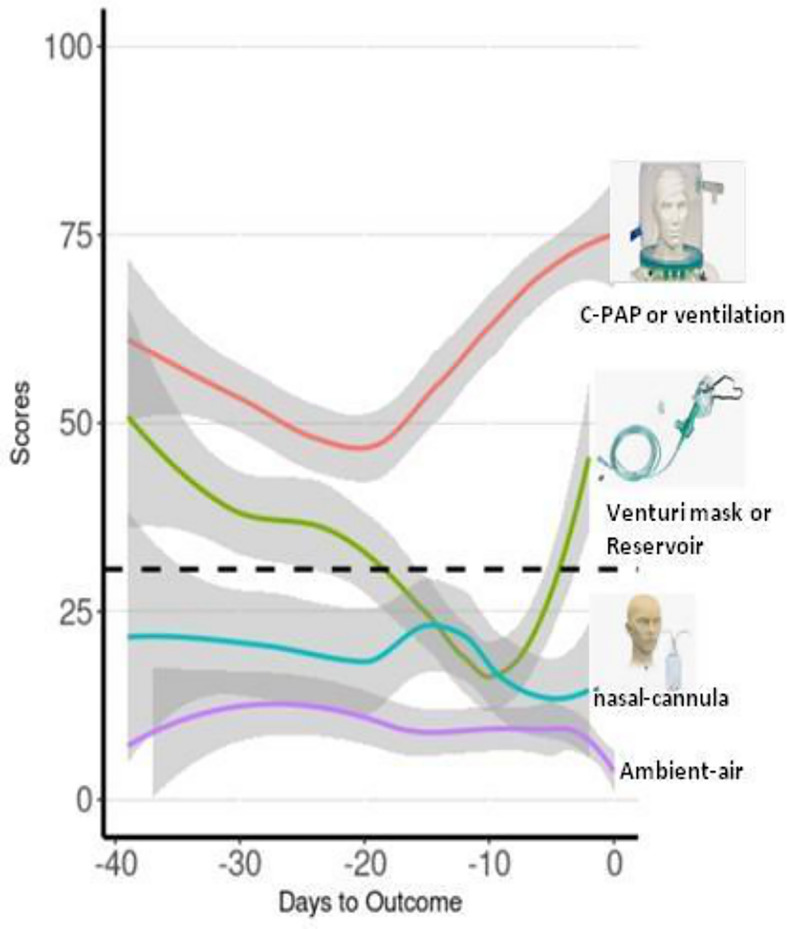
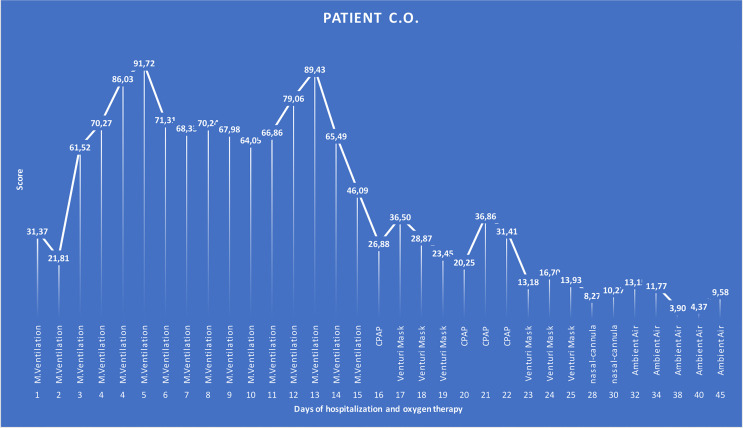
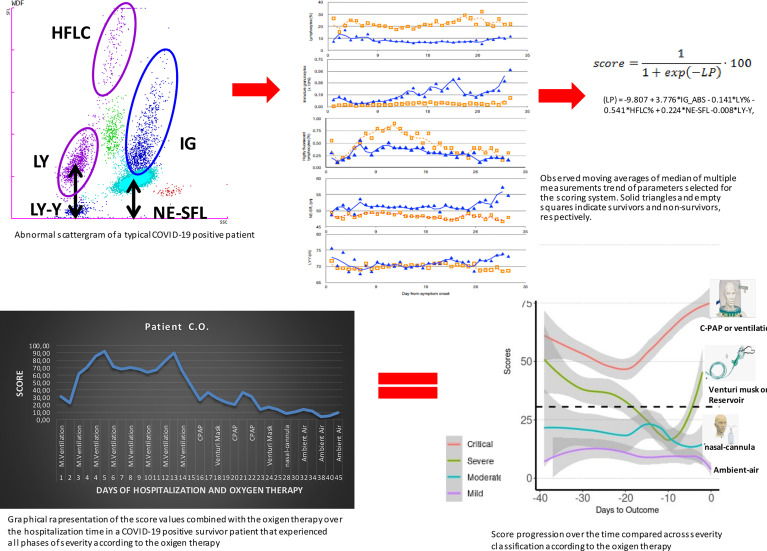
A relevant portion of patients with disease caused by the severe acute respiratory syndrome coronavirus 2 (COVID-19) experience negative outcome, and several laboratory tests have been proposed to predict disease severity. Among others, dramatic changes in peripheral blood cells have been described. We developed and validated a laboratory score solely based on blood cell parameters to predict survival in hospitalized COVID-19 patients. We retrospectively analyzed 1,619 blood cell count from 226 consecutively hospitalized COVID-19 patients to select parameters for inclusion in a laboratory score predicting severity of disease and survival. The score was derived from lymphocyte- and granulocyte-associated parameters and validated on a separate cohort of 140 consecutive COVID-19 patients. Using ROC curve analysis, a best cutoff for score of 30.6 was derived, which was associated to an overall 82.0% sensitivity (95% CI: 78-84) and 82.5% specificity (95% CI: 80-84) for detecting outcome. The scoring trend effectively separated survivor and non-survivor groups, starting 2 weeks before the end of the hospitalization period. Patients' score time points were also classified into mild, moderate, severe, and critical according to the symptomatic oxygen therapy administered. Fluctuations of the score should be recorded to highlight a favorable or unfortunate trend of the disease. The predictive score was found to reflect and anticipate the disease gravity, defined by the type of the oxygen support used, giving a proof of its clinical relevance. It offers a fast and reliable tool for supporting clinical decisions and, most important, triage in terms of not only prioritization but also allocation of limited medical resources, especially in the period when therapies are still symptomatic and many are under development. In fact, a prolonged and progressive increase of the score can suggest impaired chances of survival and/or an urgent need for intensive care unit admission.
Keywords: COVID-19 outcome; blood cell count; clinical management; immunological changes; oxygen therapy; severity score; triage.
Copyright © 2022 Birindelli, Tarkowski, Gallucci, Schiuma, Covizzi, Lewkowicz, Aloisio, Falvella, Dolci, Riva, Galli and Panteghini.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- World Health Organization . Coronavirus Disease (COVID-19) Dashboard. Data as Received by WHO From National Authorities.Available at: WHO Coronavirus (COVID-19) Dashboard | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data (Accessed Accessed: Jan 6, 2022).