

Comprehensive Metabolic Profiling of Inflammation Indicated Key Roles of Glycerophospholipid and Arginine Metabolism in Coronary Artery Disease
- PMID: 35371012
- PMCID: PMC8965586
- DOI: 10.3389/fimmu.2022.829425
Comprehensive Metabolic Profiling of Inflammation Indicated Key Roles of Glycerophospholipid and Arginine Metabolism in Coronary Artery Disease
Abstract
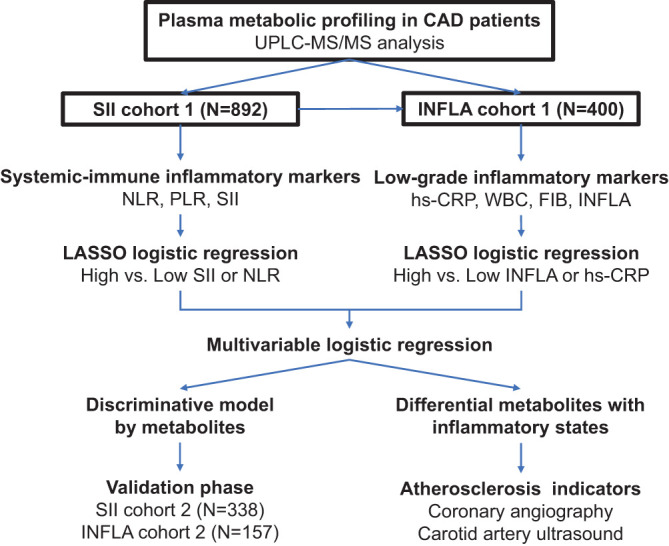
Background: Systemic immune inflammation is a key mediator in the progression of coronary artery disease (CAD), concerning various metabolic and lipid changes. In this study, the relationship between the inflammatory index and metabolic profile in patients with CAD was investigated to provide deep insights into metabolic disturbances related to inflammation.
Methods: Widely targeted plasma metabolomic and lipidomic profiling was performed in 1,234 patients with CAD. Laboratory circulating inflammatory markers were mainly used to define general systemic immune and low-grade inflammatory states. Multivariable-adjusted linear regression was adopted to assess the associations between 860 metabolites and 7 inflammatory markers. Least absolute shrinkage and selection operator (LASSO) logistic-based classifiers and multivariable logistic regression were applied to identify biomarkers of inflammatory states and develop models for discriminating an advanced inflammatory state.
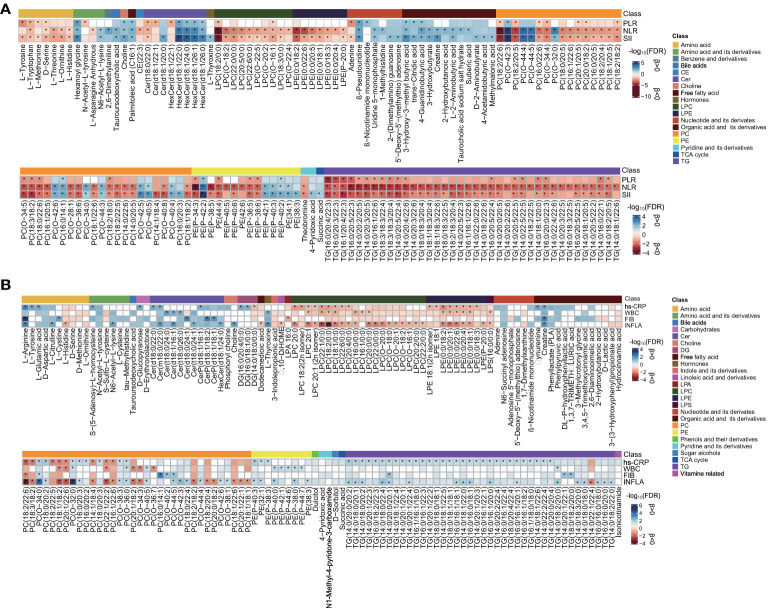
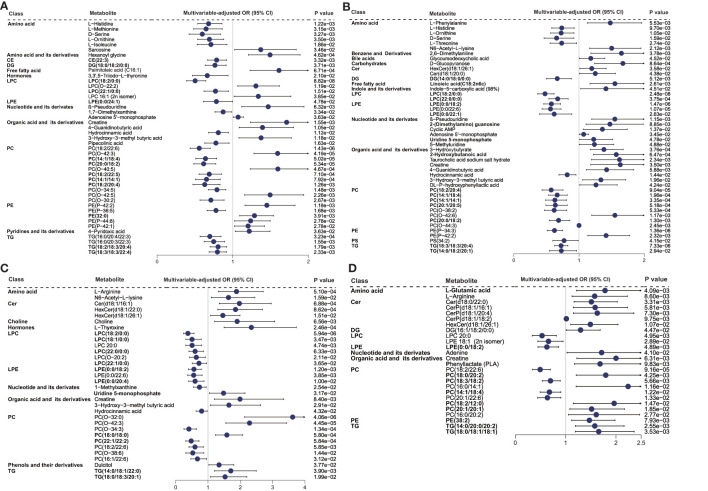
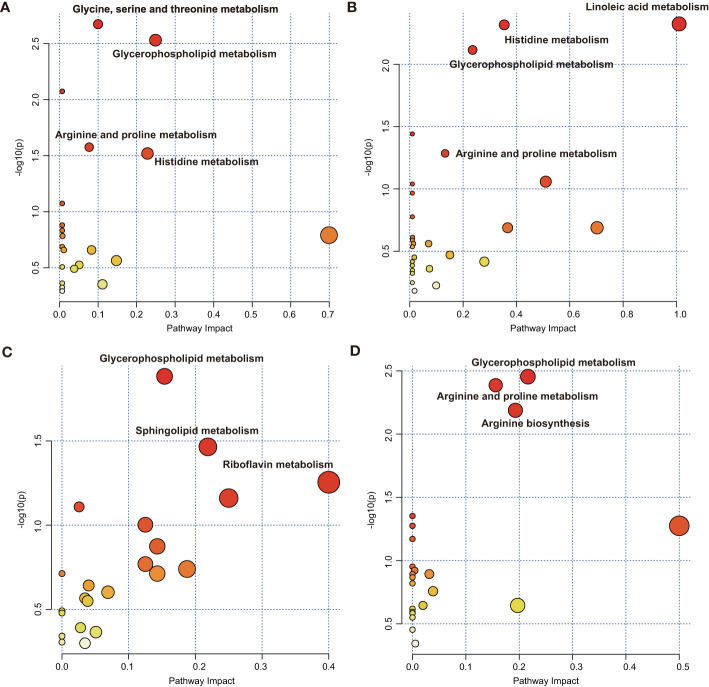
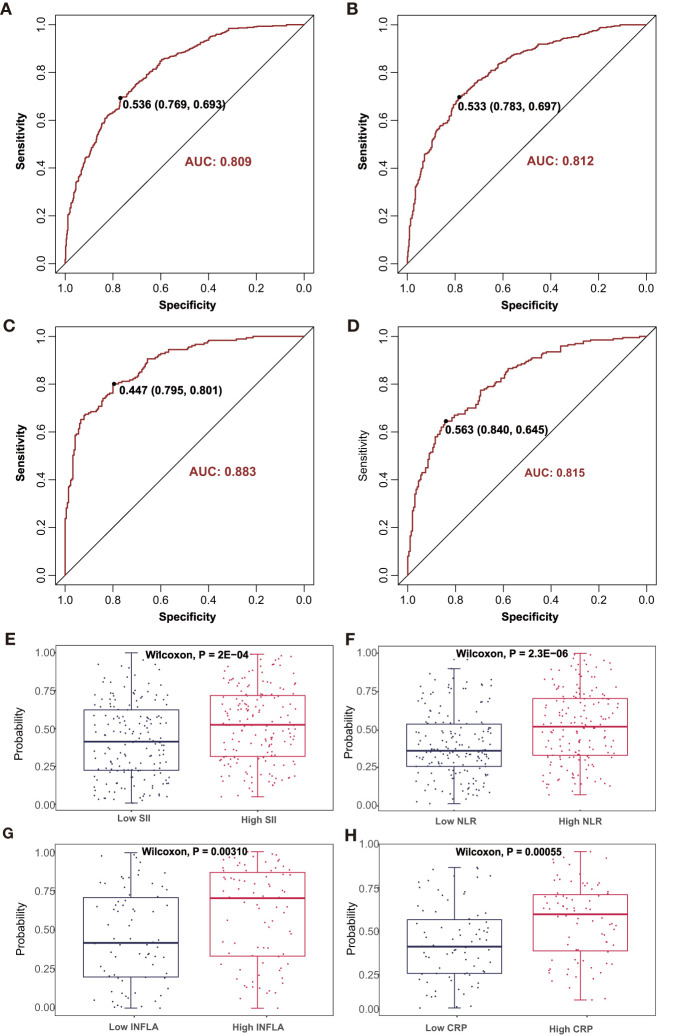
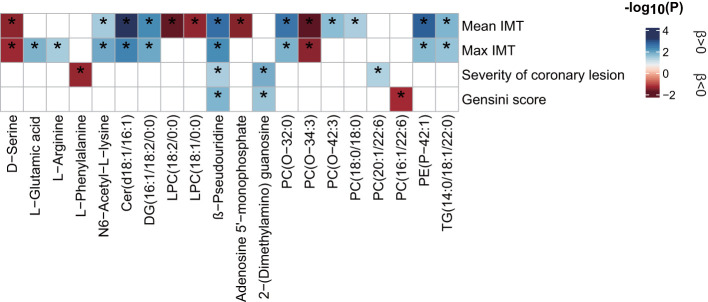
Results: Multiple metabolites and lipid species were linearly associated with the seven inflammatory markers [false discovery rate (FDR) <0.05]. LASSO and multivariable-adjusted logistic regression analysis identified significant associations between 45 metabolites and systemic immune-inflammation index, 46 metabolites and neutrophil-lymphocyte ratio states, 32 metabolites and low-grade inflammation score, and 26 metabolites and high-sensitivity C-reactive protein states (P < 0.05). Glycerophospholipid metabolism and arginine and proline metabolism were determined as key altered metabolic pathways for systemic immune and low-grade inflammatory states. Predictive models based solely on metabolite combinations showed feasibility (area under the curve: 0.81 to 0.88) for discriminating the four parameters that represent inflammatory states and were successfully validated using a validation cohort. The inflammation-associated metabolite, namely, β-pseudouridine, was related to carotid and coronary arteriosclerosis indicators (P < 0.05).
Conclusions: This study provides further information on the relationship between plasma metabolite profiles and inflammatory states represented by various inflammatory markers in CAD. These metabolic markers provide potential insights into pathological changes during CAD progression and may aid in the development of therapeutic targets.
Keywords: arteriosclerosis; coronary artery disease; glycerophospholipid metabolism; inflammation; lipidome; metabolome.
Copyright © 2022 Zhu, Wu, Mai, Guo, Meng, Fang, Chen, Liu and Zhong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Comprehensive Metabolomics Identified the Prominent Role of Glycerophospholipid Metabolism in Coronary Artery Disease Progression.Front Mol Biosci. 2021 Apr 14;8:632950. doi: 10.3389/fmolb.2021.632950. eCollection 2021. Front Mol Biosci. 2021. PMID: 33937325 Free PMC article.
-
Comprehensive Metabolomic Characterization of Coronary Artery Diseases.J Am Coll Cardiol. 2016 Sep 20;68(12):1281-93. doi: 10.1016/j.jacc.2016.06.044. J Am Coll Cardiol. 2016. PMID: 27634119
-
Association of Coronary Artery Disease and Metabolic Syndrome: Usefulness of Serum Metabolomics Approach.Front Endocrinol (Lausanne). 2021 Sep 24;12:692893. doi: 10.3389/fendo.2021.692893. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34630321 Free PMC article.
-
Metabolomics Provides Novel Insights into Epilepsy Diagnosis and Treatment: A Review.Neurochem Res. 2022 Apr;47(4):844-859. doi: 10.1007/s11064-021-03510-y. Epub 2022 Jan 24. Neurochem Res. 2022. PMID: 35067830 Review.
-
Plasma metabolites, especially lipid metabolites, are altered in pregnant women with gestational diabetes mellitus.Clin Chim Acta. 2021 Jun;517:139-148. doi: 10.1016/j.cca.2021.02.023. Epub 2021 Mar 9. Clin Chim Acta. 2021. PMID: 33711327 Review.
Cited by
-
FMT and TCM to treat diarrhoeal irritable bowel syndrome with induced spleen deficiency syndrome- microbiomic and metabolomic insights.BMC Microbiol. 2024 Oct 26;24(1):433. doi: 10.1186/s12866-024-03592-y. BMC Microbiol. 2024. PMID: 39455910 Free PMC article.
-
Coronary artery calcification is prevalent in systemic sclerosis and is associated with adverse prognosis.J Scleroderma Relat Disord. 2024 Oct;9(3):192-202. doi: 10.1177/23971983241264090. Epub 2024 Aug 11. J Scleroderma Relat Disord. 2024. PMID: 39386266
-
Integrated time-series biochemical, transcriptomic, and metabolomic analyses reveal key metabolites and signaling pathways in the liver of the Chinese soft-shelled turtle (Pelodiscus sinensis) against Aeromonas hydrophila infection.Front Immunol. 2024 May 10;15:1376860. doi: 10.3389/fimmu.2024.1376860. eCollection 2024. Front Immunol. 2024. PMID: 38799475 Free PMC article.
-
Active dry yeast enhances immunity through modulation of gut microbiota and serum metabolic processes in captive forest musk deer (Moschus berezovskii).BMC Vet Res. 2025 Apr 12;21(1):262. doi: 10.1186/s12917-025-04705-z. BMC Vet Res. 2025. PMID: 40221712 Free PMC article.
-
Recent Advances and Perspectives of Metabolomics-Based Investigations in Coronary Heart Disease.Curr Atheroscler Rep. 2025 Jun 9;27(1):63. doi: 10.1007/s11883-025-01304-z. Curr Atheroscler Rep. 2025. PMID: 40488965 Review.
References
-
- Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO, Criqui M, et al. . Markers of Inflammation and Cardiovascular Disease: Application to Clinical and Public Health Practice: A Statement for Healthcare Professionals From the Centers for Disease Control and Prevention and the American Heart Association. Circulation (2003) 107:499–511. doi: 10.1161/01.cir.0000052939.59093.45 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous