

HLA-B*13, B*35 and B*39 Alleles Are Closely Associated With the Lack of Response to ART in HIV Infection: A Cohort Study in a Population of Northern Brazil
- PMID: 35371095
- PMCID: PMC8966405
- DOI: 10.3389/fimmu.2022.829126
HLA-B*13, B*35 and B*39 Alleles Are Closely Associated With the Lack of Response to ART in HIV Infection: A Cohort Study in a Population of Northern Brazil
Abstract
Introduction: Immune reconstitution failure after HIV treatment is a multifactorial phenomenon that may also be associated with a single polymorphism of human leukocyte antigen (HLA); however, few reports include patients from the Brazilian Amazon. Our objective was to evaluate the association of the immunogenic profile of the "classical" HLA-I and HLA-II loci with treatment nonresponse in a regional cohort monitored over 24 months since HIV diagnosis.
Materials and methods: Treatment-free participants from reference centers in the state of Pará, Brazil, were enrolled. Infection screening was performed using enzyme immunoassays (Murex AG/AB Combination DiaSorin, UK) and confirmed by immunoblots (Bio-Manguinhos, FIOCRUZ). Plasma viral load was quantified by real-time PCR (ABBOTT, Chicago, Illinois, USA). CD4+/CD8+ T lymphocyte quantification was performed by immunophenotyping and flow cytometry (BD Biosciences, San Jose, CA, USA). Infection was monitored via test and logistics platforms (SISCEL and SICLOM). Therapeutic response failure was inferred based on CD4+ T lymphocyte quantification after 1 year of therapy. Loci A, B and DRB1 were genotyped using PCR-SSO (One Lambda Inc., Canoga Park, CA, USA). Statistical tests were applied using GENEPOP, GraphPad Prism 8.4.3 and BioEstat 5.3.
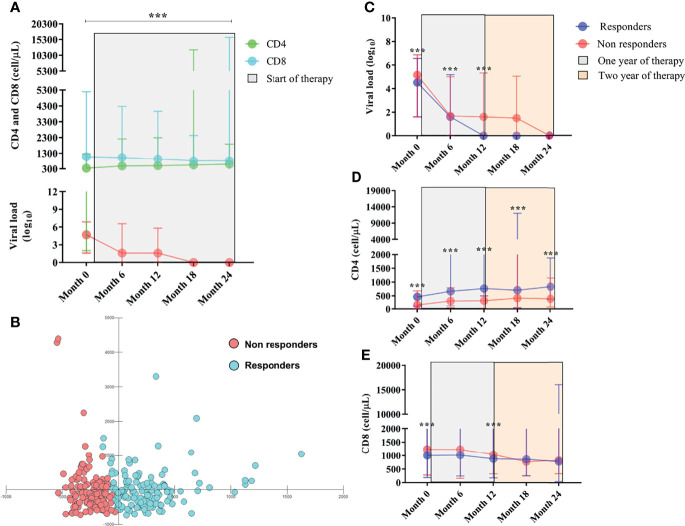
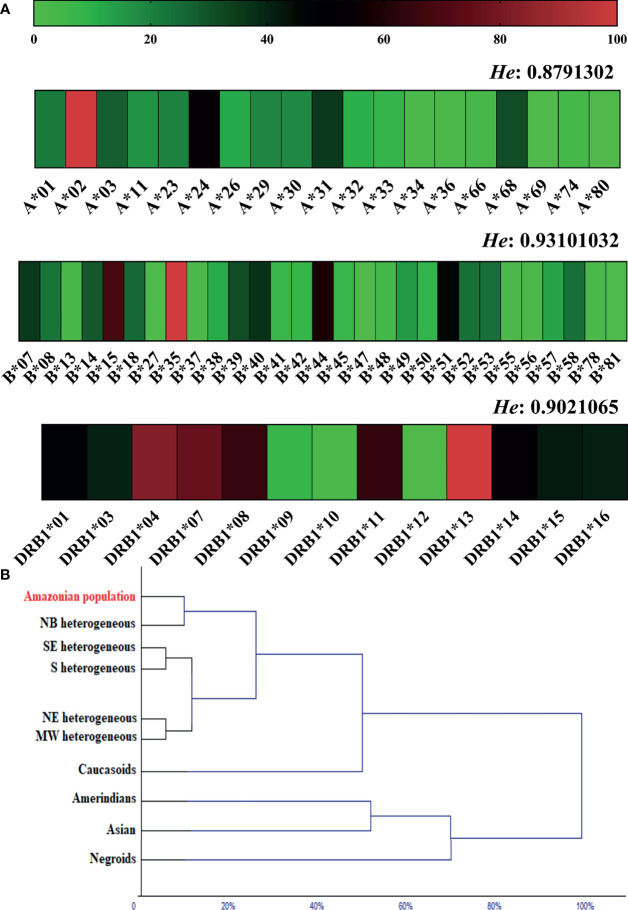
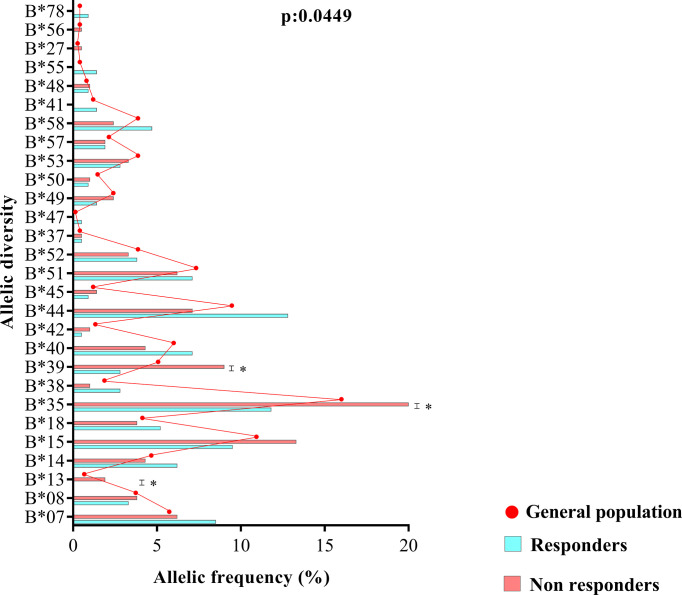
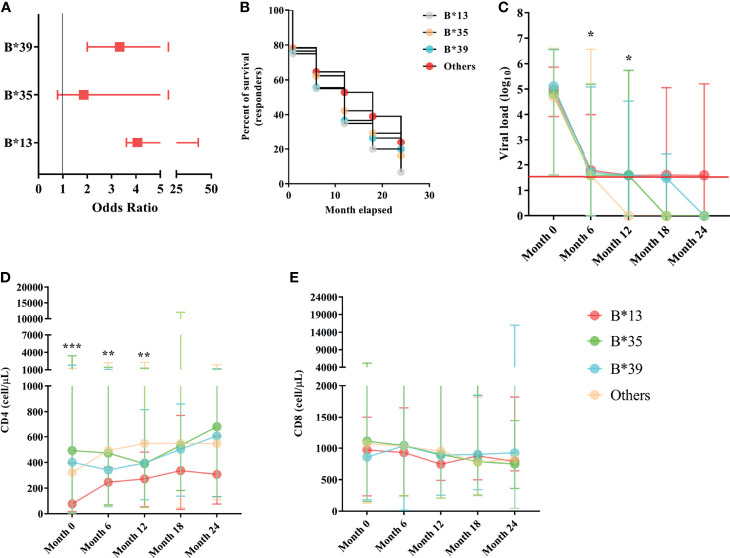
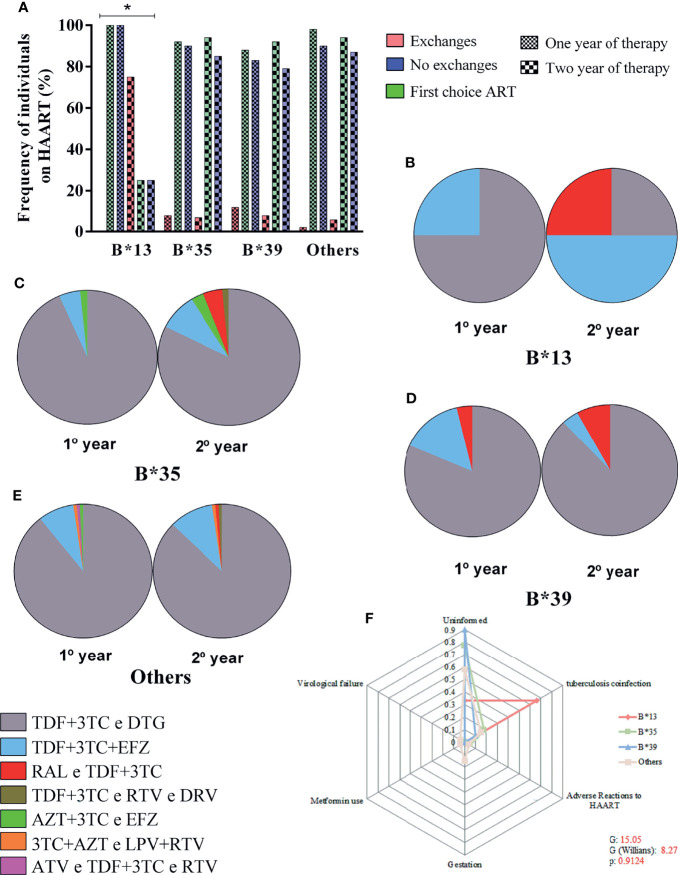
Results: Of the 270 patients monitored, 134 responded to treatment (CD4+ ≥ 500 cells/µL), and 136 did not respond to treatment (CD4+ < 500 cells/µL). The allele frequencies of the loci were similar to heterogeneous populations. The allelic profile of locus B was statistically associated with treatment nonresponse, and the B*13, B*35 and B*39 alleles had the greatest probabilistic influence. The B*13 allele had the highest risk of treatment nonresponse, and carriers of the allele had a detectable viral load and a CD4+ T lymphocyte count less than 400 cells/µL with up to 2 years of therapy. The B*13 allele was associated with a switch in treatment regimens, preferably to efavirenz (EFZ)-based regimens, and among those who switched regimens, half had a history of coinfection with tuberculosis.
Conclusions: The allelic variants of the B locus are more associated with non-response to therapy in people living with HIV (PLHIV) from a heterogeneous population in the Brazilian Amazon.
Keywords: B*13; HIV; HLA; immunogenetics; therapeutic response.
Copyright © 2022 Pereira, França, Costa, Jorge, Mattos, Freire, Ramos, Monteiro, Macedo, Sousa, Santos, Freitas, Costa and Vallinoto.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Lewden C, Chene G, Morlat P, Raffi F, Dupon M, Dellamonica P, et al. . HIV-Infected Adults With a CD4 Cell Count Greater Than 500 Cells/Mm3 on Long-Term Combination Antiretroviral Therapy Reach Same Mortality Rates as the General Population. J Acquir Immune Defic Syndr (2007) 46(1):72–7. doi: 10.1097/QAI.0b013e318134257a - DOI - PubMed
-
- Tanaskovic S, Fernandez S, French MA, Price RI, Song S, Robins PD, et al. . Thymic Tissue Is Not Evident on High-Resolution Computed Tomography and [¹⁸F]fluoro-Deoxy-Glucose Positron Emission Tomography Scans of Aviraemic HIV Patients With Poor Recovery of CD4⁺ T Cells. AIDS (2011) 25(9):1235–7. doi: 10.1097/QAD.0b013e3283474155 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials