

The Burden of Critical Illness in Hospitalized Children in Low- and Middle-Income Countries: Protocol for a Systematic Review and Meta-Analysis
- PMID: 35372149
- PMCID: PMC8970052
- DOI: 10.3389/fped.2022.756643
The Burden of Critical Illness in Hospitalized Children in Low- and Middle-Income Countries: Protocol for a Systematic Review and Meta-Analysis
Abstract
Background: The majority of childhood deaths occur in low- and middle-income countries (LMICs). Many of these deaths are avoidable with basic critical care interventions. Quantifying the burden of pediatric critical illness in LMICs is essential for targeting interventions to reduce childhood mortality.
Objective: To determine the burden of hospitalization and mortality associated with acute pediatric critical illness in LMICs through a systematic review and meta-analysis of the literature.
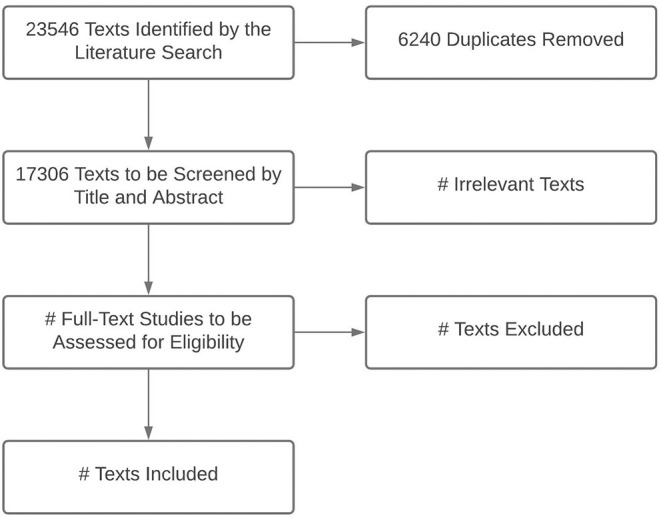
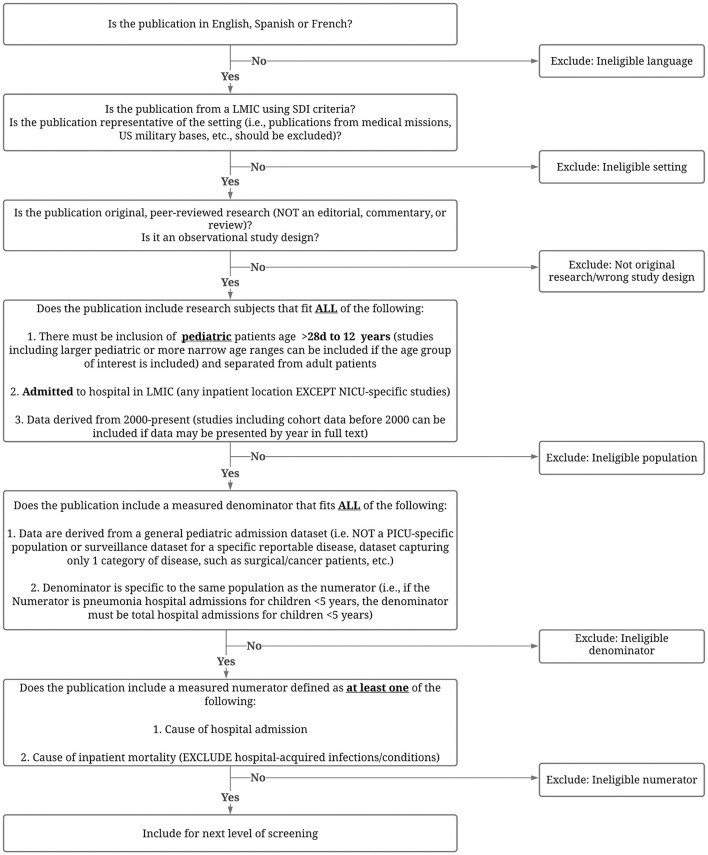
Data sources and search strategy: We will identify eligible studies by searching MEDLINE, EMBASE, CINAHL, and LILACS using MeSH terms and keywords. Results will be limited to infants or children (ages >28 days to 12 years) hospitalized in LMICs and publications in English, Spanish, or French. Publications with non-original data (e.g., comments, editorials, letters, notes, conference materials) will be excluded.
Study selection: We will include observational studies published since January 1, 2005, that meet all eligibility criteria and for which a full text can be located.
Data extraction: Data extraction will include information related to study characteristics, hospital characteristics, underlying population characteristics, patient population characteristics, and outcomes.
Data synthesis: We will extract and report data on study, hospital, and patient characteristics; outcomes; and risk of bias. We will report the causes of admission and mortality by region, country income level, and age. We will report or calculate the case fatality rate (CFR) for each diagnosis when data allow.
Conclusions: By understanding the burden of pediatric critical illness in LMICs, we can advocate for resources and inform resource allocation and investment decisions to improve the management and outcomes of children with acute pediatric critical illness in LMICs.
Keywords: child health; critical illness; global health; hospitalization; low- and middle-income countries (LMIC); pediatrics—children; resource limited setting.
Copyright © 2022 Kortz, Nielsen, Mediratta, Reeves, O'Brien, Lee, Attebery, Bhutta, Biewen, Coronado Munoz, deAlmeida, Fonseca, Hooli, Johnson, Kissoon, Leimanis-Laurens, McCarthy, Pineda, Remy, Sanders, Takwoingi, Wiens, Bhutta and The Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network on Behalf of the PALISI Global Health Subgroup.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer YHM declared a shared affiliation with one of the authors JL to the handling editor at the time of review.
Figures
References
-
- Reiner RC, Jr., Olsen HE, Ikeda CT, Echko MM, Ballestreros KE, Manguerra H, et al. Diseases, injuries, and risk factors in child and adolescent health, 1990 to 2017: findings from the global burden of diseases, injuries, and risk factors 2017 study. JAMA pediatr. (2019). 173:e190337. 10.1001/jamapediatrics.2019.0337 - DOI - PMC - PubMed
-
- Institute for Health Metrics and Evaluation (IHME) . Findings from the Global Burden of Disease Study 2017. Seattle, WA: IHME; (2018).