Accessory and Expiratory Muscles Activation During Spontaneous Breathing Trial: A Physiological Study by Surface Electromyography
- PMID: 35372418
- PMCID: PMC8965594
- DOI: 10.3389/fmed.2022.814219
Accessory and Expiratory Muscles Activation During Spontaneous Breathing Trial: A Physiological Study by Surface Electromyography
Abstract
Background: The physiological and prognostical significance of accessory and expiratory muscles activation is unknown during a spontaneous breathing trial (SBT). We hypothesized that, in patients experiencing weaning failure, accessory and expiratory muscles are activated to cope with an increased respiratory workload.
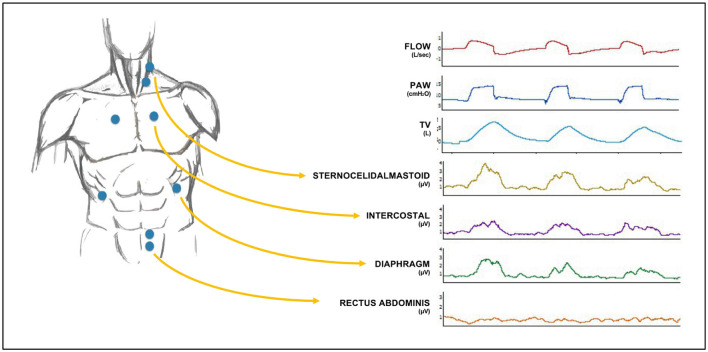
Purpose: To describe accessory and expiratory muscle activation non-invasively by surface electromyography (sEMG) during an SBT and to assess differences in electrical activity (EA) of the inspiratory and expiratory muscles in successful vs. failing weaning patients.
Methods: Intubated patients on mechanical ventilation for more than 48 h undergoing an SBT were enrolled in a medical and surgical third-level ICU of the University Teaching Hospital. Baseline characteristics and physiological variables were recorded in a crossover physiologic prospective clinical study.
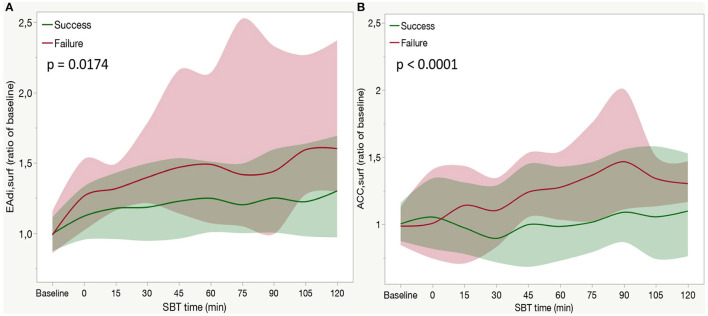
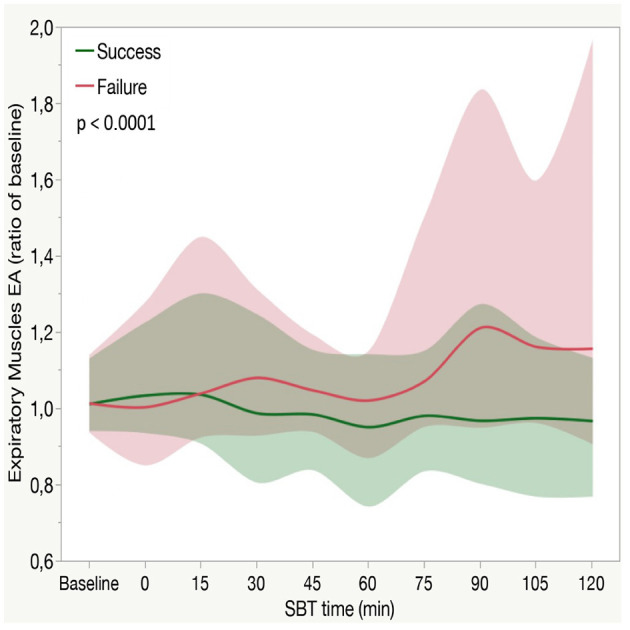
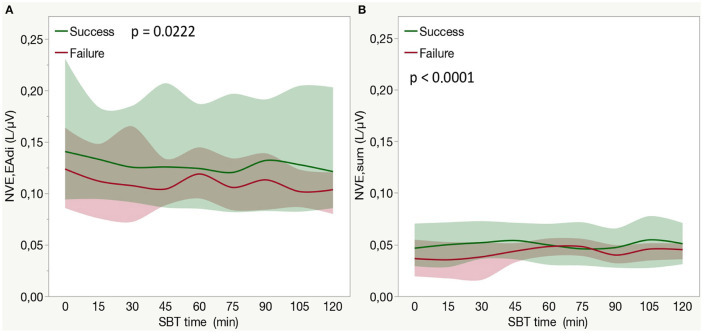
Results: Of 37 critically ill mechanically ventilated patients, 29 (78%) patients successfully passed the SBT. Rapid shallow breathing index (RSBI) was higher in patients who failed SBT compared with the successfully weaned patients at baseline and over time (group-by-time interaction p < 0.001). EA of both the diaphragm (EAdisurf) and of accessory muscles (ACCsurf) was higher in failure patients compared with success (group-by-time interaction p = 0.0174 and p < 0.001, respectively). EA of expiratory muscles (ESPsurf) during SBT increased more in failure than in weaned patients (group-by-time interaction p < 0.0001).
Conclusion: Non-invasive respiratory muscle monitoring by sEMG was feasible during SBT. Respiratory muscles EA increased during SBT, regardless of SBT outcome, and patients who failed the SBT had a higher increase of all the inspiratory muscles EA compared with the patients who passed the SBT. Recruitment of expiratory muscles-as quantified by sEMG-is associated with SBT failure.
Keywords: electrical activity; expiratory muscles; inspiratory muscles; non-invasive surface electromyography; spontaneous breathing trial (SBT); weaning.
Copyright © 2022 Pozzi, Rezoagli, Bronco, Rabboni, Grasselli, Foti and Bellani.
Conflict of interest statement
GB was employed by Draeger Medical Italy, Draeger Medical Germany, and Pfizer. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures