

Acute Kidney Injury Associated with Coronavirus Disease 2019 in Urban New Orleans
- PMID: 35372932
- PMCID: PMC8815549
- DOI: 10.34067/KID.0002652020
Acute Kidney Injury Associated with Coronavirus Disease 2019 in Urban New Orleans
Abstract
Background: AKI is a manifestation of COVID-19 (CoV-AKI). However, there is paucity of data from the United States, particularly from a predominantly black population. We report the phenotype and outcomes of AKI at an academic hospital in New Orleans.
Methods: We conducted an observational study in patients hospitalized at Ochsner Medical Center over a 1-month period with COVID-19 and diagnosis of AKI (KDIGO). We examined the rates of RRT and in-hospital mortality as outcome measures.
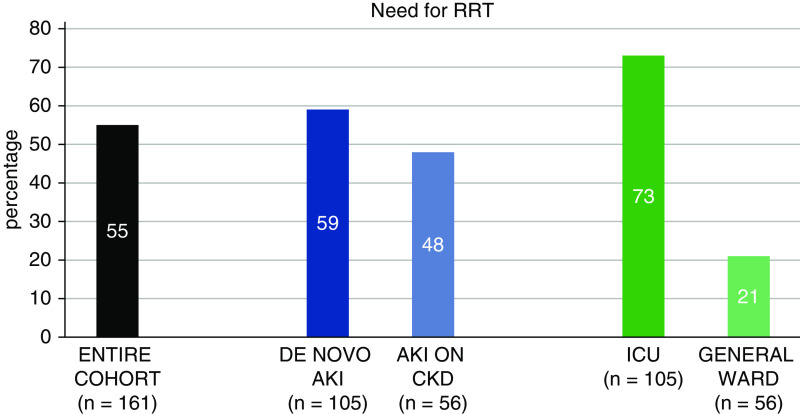
Results: Among 575 admissions (70% black) with COVID-19 [173 (30%) to an intensive care unit (ICU)], we found 161 (28%) cases of AKI (61% ICU and 14% general ward admissions). Patients were predominantly men (62%) and hypertensive (83%). Median body mass index (BMI) was higher among those with AKI (34 versus 31 kg/m2, P<0.0001). AKI over preexisting CKD occurred in 35%. Median follow-up was 25 (1-45) days. The in-hospital mortality rate for the AKI cohort was 50%. Vasopressors and/or mechanical ventilation were required in 105 (65%) of those with AKI. RRT was required in 89 (55%) patients. Those with AKI requiring RRT (AKI-RRT) had higher median BMI (35 versus 33 kg/m2, P=0.05) and younger age (61 versus 68, P=0.0003). Initial values of ferritin, C-reactive protein, procalcitonin, and lactate dehydrogenase were higher among those with AKI; and among them, values were higher for those with AKI-RRT. Ischemic acute tubular injury (ATI) and rhabdomyolysis accounted for 66% and 7% of causes, respectively. In 13%, no obvious cause of AKI was identified aside from COVID-19 diagnosis.
Conclusions: CoV-AKI is associated with high rates of RRT and death. Higher BMI and inflammatory marker levels are associated with AKI as well as with AKI-RRT. Hemodynamic instability leading to ischemic ATI is the predominant cause of AKI in this setting.
Keywords: COVID-19; ICU; New Orleans; SARS; SARS-CoV-2; United States; acute kidney injury; acute kidney injury and ICU nephrology; black; dialysis; hospital mortality; obesity; phenotype; proteinuria; renal replacement therapy.
Copyright © 2020 by the American Society of Nephrology.
Conflict of interest statement
J.C. Velez has participated in Advisory Board engagements with Mallinckrodt Pharmaceuticals and Retrophin, and has been a member of a Speaker Bureau for Otsuka Pharmaceuticals. All remaining authors have nothing to disclose.
Figures




Comment in
- 588–590 doi: 10.34067/KID.0003722020
References
-
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao GF, Tan W; China Novel Coronavirus Investigating and Research Team : A novel coronavirus from patients with Pneumonia in China, 2019. N Engl J Med 382: 727–733, 2020 - PMC - PubMed
-
- Available at: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html. Accessed April 15, 2020
-
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B: Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [published correction appears in Lancet 395:496, 2020]. Lancet 395: 497–506, 2020 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
