

Opportunities To Improve Diabetes Care in the Hemodialysis Unit: A Cohort Study in Ontario, Canada
- PMID: 35373046
- PMCID: PMC8791316
- DOI: 10.34067/KID.0007082020
Opportunities To Improve Diabetes Care in the Hemodialysis Unit: A Cohort Study in Ontario, Canada
Abstract
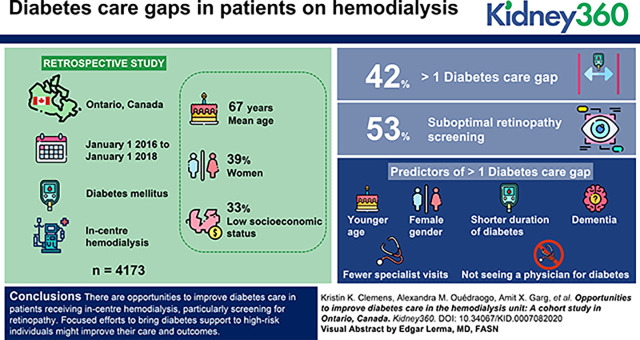
Background: Patients with diabetes receiving chronic, in-center hemodialysis face healthcare challenges. We examined the prevalence of gaps in their diabetes care, explored regional differences, and determined predictors of care gaps.
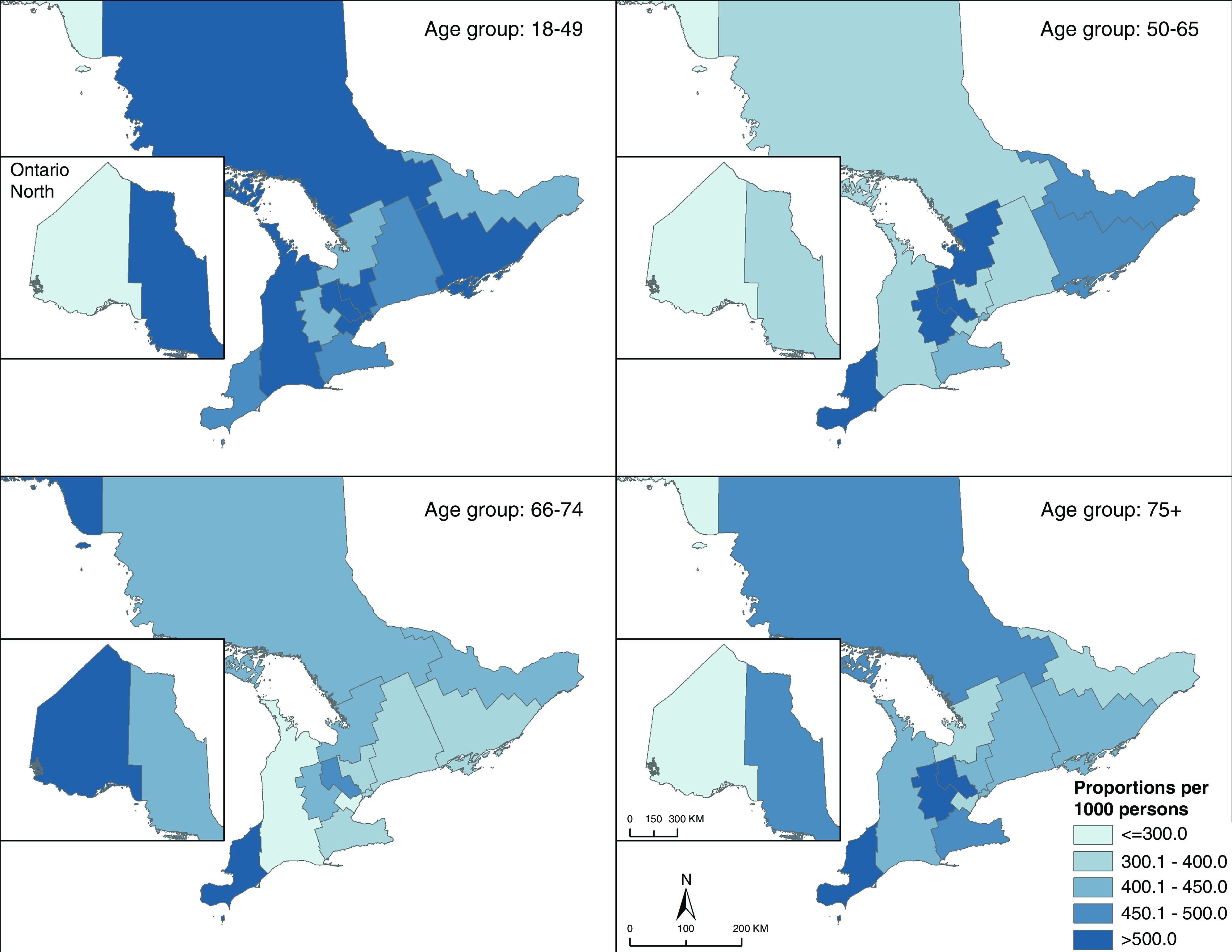
Methods: We conducted a population-based, retrospective study between January 1, 2016 and January 1, 2018 in Ontario, Canada. We included adults with prevalent diabetes mellitus receiving in-center hemodialysis as of January 1, 2018 and examined the proportion with (1) insufficient or excessive glycemic monitoring, (2) suboptimal screening for diabetes-related complications (retinopathy and cardiovascular screening), (3) hospital encounters for hypo- or hyperglycemia, and (4) hospital encounters for hypertension in the 2 years prior (January 1, 2016 to January 1, 2018). We then identified patient, provider, and health-system factors associated with more than one care gap and used multivariable logistic regression to determine predictors. Further, we used geographic information systems to explore spatial variation in gaps.
Results: There were 4173 patients with diabetes receiving in-center hemodialysis; the mean age was 67 years, 39% were women, and the majority were of lower socioeconomic status. Approximately 42% of patients had more than one diabetes care gap, the most common being suboptimal retinopathy screening (53%). Significant predictors of more than one gap included younger age, female sex, shorter duration of diabetes, dementia, fewer specialist visits, and not seeing a physician for diabetes. There was evidence of spatial variation in care gaps across our region.
Conclusions: There are opportunities to improve diabetes care in patients receiving in-center hemodialysis, particularly screening for retinopathy. Focused efforts to bring diabetes support to high-risk individuals might improve their care and outcomes.
Keywords: Ontario; chronic hemodialysis; cohort studies; diabetes and the kidney; diabetes mellitus; hemodialysis units; quality of care.
Copyright © 2021 by the American Society of Nephrology.
Conflict of interest statement
K.K. Clemens received a diabetes research award sponsored by AstraZeneca; honoraria for delivering certified continuing medical education talks from the Canadian Medical and Surgical Knowledge Translation Research Group and Sutherland Global Services Canada ULC; and has attended Merck-sponsored conferences. A.X. Garg reports being on the editorial boards of American Journal of Kidney Diseases and Kidney International; receiving research funding from Astellas; serving on the data safety and monitoring board for an investigator-initiated trial program funded by GlaxoSmithKline; and serving as medical lead role to improve access to kidney transplantation and living kidney donation for the Ontario Renal Network (government-funded agency located within Ontario Health). S. Silver reports receiving honoraria from Baxter and Sanofi and serving on the editorial board of the Canadian Journal of Kidney Health and Disease. All remaining authors have nothing to disclose.
Figures
References
-
- Canadian Institute for Health Information: Access data and reports. Available at: https://www.cihi.ca/en/access-data-reports/results?query=Treatment+of+En.... Accessed January 22, 2021
-
- Pugliese G, Solini A, Bonora E, Orsi E, Zerbini G, Fondelli C, Gruden G, Cavalot F, Lamacchia O, Trevisan R, Vedovato M, Penno G; RIACE Study Group: Distribution of cardiovascular disease and retinopathy in patients with type 2 diabetes according to different classification systems for chronic kidney disease: A cross-sectional analysis of the renal insufficiency and cardiovascular events (RIACE) Italian multicenter study. Cardiovasc Diabetol 13: 59, 2014. 10.1186/1475-2840-13-59 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
