

Adding Life to Their Years: The Current State of Pediatric Palliative Care in CKD
- PMID: 35373080
- PMCID: PMC8791371
- DOI: 10.34067/KID.0000282021
Adding Life to Their Years: The Current State of Pediatric Palliative Care in CKD
Abstract
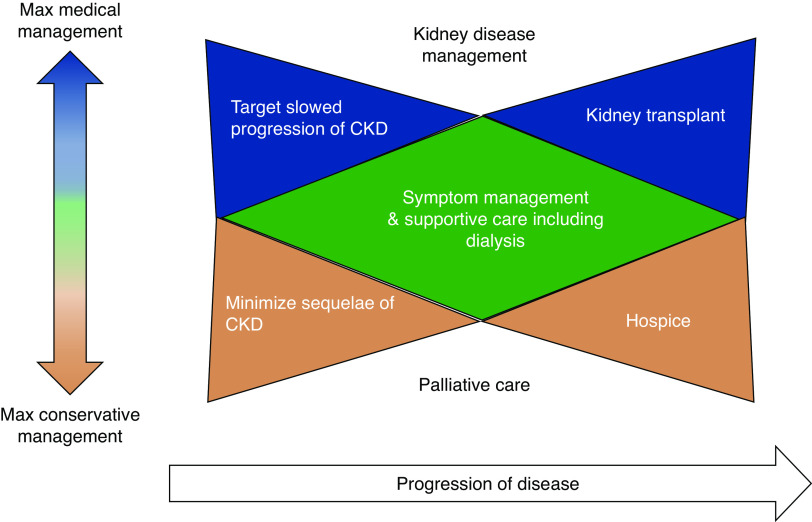
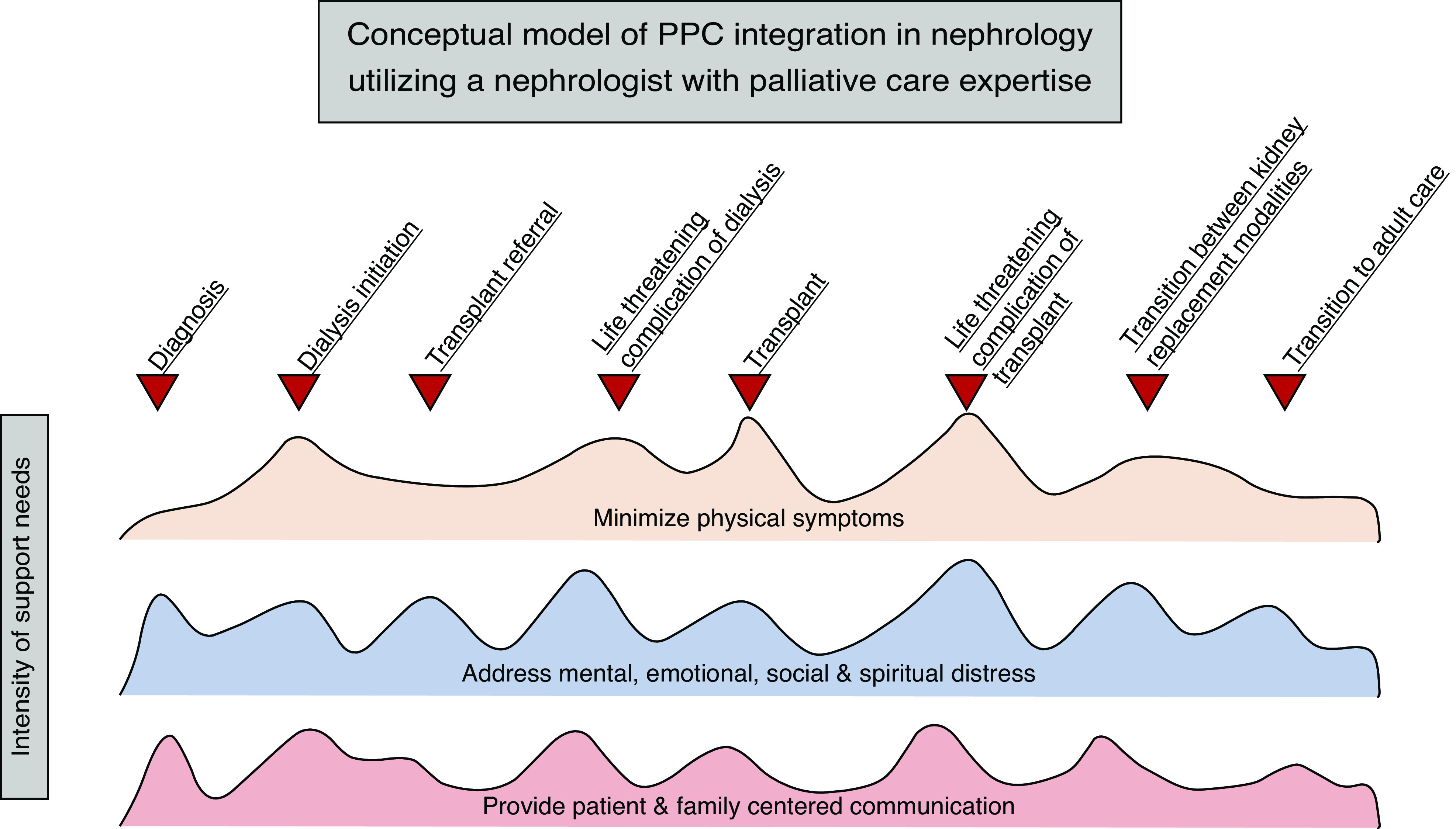
Despite continued advances in medical treatment, pediatric CKD remains an unremitting, burdensome condition characterized by decreased quality of life and earlier death. These burdens underscore the need for integration of pediatric palliative care (PPC) into nephrology practice. PPC is an evolving field that strives to (1) relieve physical, psychologic, social, practical, and existential suffering; (2) improve quality of life; (3) facilitate decision making; and (4) assist with care coordination in children with life-threatening or life-shortening conditions. Integration of palliative care into routine care has already begun for adults with kidney disease and children with other chronic diseases; however, similar integration has not occurred in pediatric nephrology. This review serves to provide a comprehensive definition of PPC, highlight the unmet need in pediatric nephrology and current integration efforts, discuss the state of palliative care in adult nephrology and analogous chronic pediatric disease states, and introduce future opportunities for study.
Keywords: chronic kidney disease; dialysis; end stage kidney disease; geriatric and palliative nephrology; kidney supportive care; pediatric nephrology; pediatric palliative care.
Copyright © 2021 by the American Society of Nephrology.
Conflict of interest statement
Dr. House is supported by a National Institutes of Health training grant (5T32DK007662-30, P I Hingorani). The remaining author has nothing to disclose.
Figures
References
-
- Buyan N, Türkmen MA, Bilge I, Baskin E, Haberal M, Bilginer Y, Mir S, Emre S, Akman S, Ozkaya O, Fidan K, Alpay H, Kavukcu S, Sever L, Ozçakar ZB, Dogrucan N: Quality of life in children with chronic kidney disease (with child and parent assessments). Pediatr Nephrol 25: 1487–1496, 2010. 10.1007/s00467-010-1486-1 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
