

The 2021 WHO catalogue of Mycobacterium tuberculosis complex mutations associated with drug resistance: A genotypic analysis
- PMID: 35373160
- PMCID: PMC7612554
- DOI: 10.1016/S2666-5247(21)00301-3
The 2021 WHO catalogue of Mycobacterium tuberculosis complex mutations associated with drug resistance: A genotypic analysis
Abstract
Background: Molecular diagnostics are considered the most promising route to achieving rapid, universal drug susceptibility testing for Mycobacterium tuberculosiscomplex (MTBC). We aimed to generate a WHO endorsed catalogue of mutations to serve as a global standard for interpreting molecular information for drug resistance prediction.
Methods: A candidate gene approach was used to identify mutations as associated with resistance, or consistent with susceptibility, for 13 WHO endorsed anti-tuberculosis drugs. 38,215 MTBC isolates with paired whole-genome sequencing and phenotypic drug susceptibility testing data were amassed from 45 countries. For each mutation, a contingency table of binary phenotypes and presence or absence of the mutation computed positive predictive value, and Fisher's exact tests generated odds ratios and Benjamini-Hochberg corrected p-values. Mutations were graded as Associated with Resistance if present in at least 5 isolates, if the odds ratio was >1 with a statistically significant corrected p-value, and if the lower bound of the 95% confidence interval on the positive predictive value for phenotypic resistance was >25%. A series of expert rules were applied for final confidence grading of each mutation.
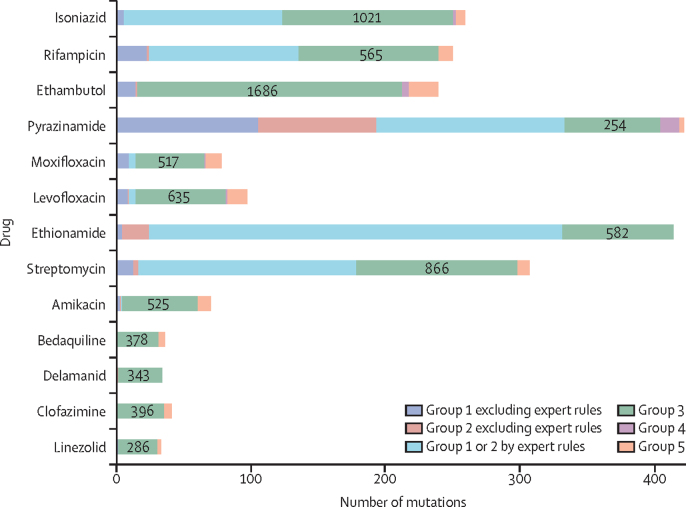
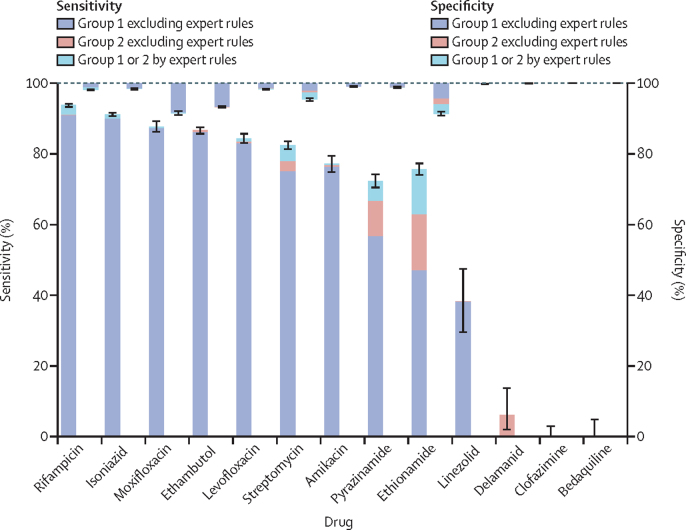
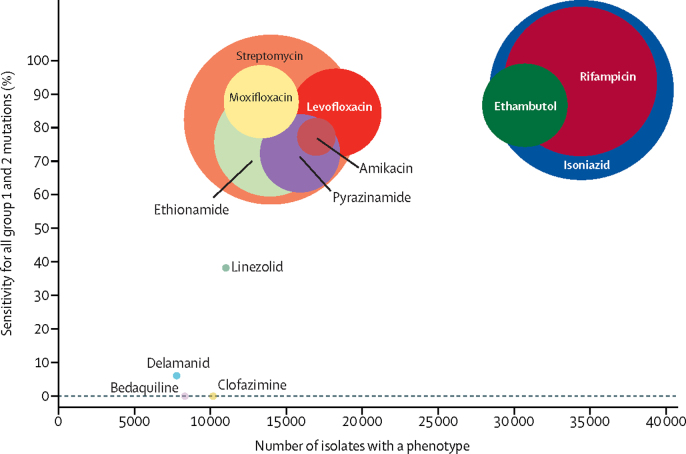
Findings: 15,667 associations were computed for 13,211 unique mutations linked to one or more drugs. 1,149/15,667 (7·3%) mutations were classified as associated with phenotypic resistance and 107/15,667 (0·7%) were deemed consistent with susceptibility. For rifampicin, isoniazid, ethambutol, fluoroquinolones, and streptomycin, the mutations' pooled sensitivity was >80%. Specificity was over 95% for all drugs except ethionamide (91·4%), moxifloxacin (91·6%) and ethambutol (93·3%). Only two resistance mutations were classified for bedaquiline, delamanid, clofazimine, and linezolid as prevalence of phenotypic resistance was low for these drugs.
Interpretation: This first WHO endorsed catalogue of molecular targets for MTBC drug susceptibility testing provides a global standard for resistance interpretation. Its existence should encourage the implementation of molecular diagnostics by National Tuberculosis Programmes.
Funding: UNITAID, Wellcome, MRC, BMGF.
Conflict of interest statement
Conflicts of interest C.U.K. is a consultant Becton Dickinson, the Foundation for Innovative New Diagnostics and the TB Alliance. C.U.K. is collaborating with Janssen, PZA Innovation and Thermo Fisher Scientific. C.U.K. worked as a consultant for QuantuMDx, the Stop TB Partnership, the World Health Organization (WHO) Global TB Programme and the WHO Regional Office for Europe. C.U.K. gave a paid educational talk for Oxford Immunotec. Hain Lifescience covered C.U.K.’s and accommodation to present at a meeting. C.U.K. is an unpaid advisor to BioVersys and GenoScreen. E.R. is employed by Public Health England and holds an honorary contract with Imperial College London. I.F.L. is Director of the Scottish Mycobacteria Reference Laboratory. S.N. receives funding from German Center for Infection Research, Excellenz Cluster Precision Medicine in Chronic Inflammation, Leibniz Science Campus Evolutionary Medicine of the LUNG (EvoLUNG)tion EXC 2167. P.S. is a consultant at Genoscreen. T.R. is funded by NIH and DoD and receives salary support from the non-profit organization FIND. T.R. is a co-founder, board member and shareholder of Verus Diagnostics Inc, a company that was founded with the intent of developing diagnostic assays. Verus Diagnostics was not involved in any way with data collection, analysis or publication of the results. T.R. has not received any financial support from Verus Diagnostics. UCSD Conflict of Interest office has reviewed and approved T.R.’s role in Verus Diagnostics Inc. T.R. is a co-inventor of a provisional patent for a TB diagnostic assay (provisional patent #: 63/048.989). T.R. is a co-inventor on a patent associated with the processing of TB sequencing data (European Patent Application No. 14840432.0 & USSN 14/912,918). T.R. has agreed to “donate all present and future interest in and rights to royalties from this patent” to UCSD to ensure that he does not receive any financial benefits from this patent. S.S. is working and holding ESOPs at HaystackAnalytics Pvt. Ltd. (Product: Using whole genome sequencing for drug susceptibility testing for Mycobacterium tuberculosis). G.F.G. is listed as an inventor on patent applications for RBD-dimer-based CoV vaccines. The patents for RBD-dimers as protein subunit vaccines for SARS-CoV-2 have been licensed to Anhui Zhifei Longcom Biopharmaceutical Co. Ltd, China. No other authors declare a conflict of interest. I.C. is a consultant for the Foundation for Innovative New Diagnostics. DAC reports funding from GlaxoSmithKline and consultancy fees from Biobeats, Oxford University Innovation, Sensyne Health.C.C. reports funding from FIND to his institution (Pathology Queensland, Queensland Department of Health) for his laboratory to perform molecular analytic studies (limits of detection) for new molecular platforms manufactured by Cepheid and Bioneer.
Figures
Comment in
-
Assessment of the 2021 WHO Mycobacterium tuberculosis drug resistance mutation catalogue on an independent dataset.Lancet Microbe. 2022 Sep;3(9):e645. doi: 10.1016/S2666-5247(22)00151-3. Epub 2022 May 31. Lancet Microbe. 2022. PMID: 35659881 No abstract available.
References
-
- WHO Impact of the COVID-19 pandemic on TB detection and mortality in 2020. 2021. https://cdn.who.int/media/docs/default-source/hq-tuberculosis/impact-of-...
-
- WHO Global tuberculosis report, 2020. 2020. https://apps.who.int/iris/handle/10665/336069
-
- WHO Meeting report of the WHO expert consultation on the definition of extensively drug-resistant tuberculosis. 2020. https://apps.who.int/iris/handle/10665/338776
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
