

Meniscal Treatment as a Predictor of Worse Articular Cartilage Damage on MRI at 2 Years After ACL Reconstruction: The MOON Nested Cohort
- PMID: 35373606
- PMCID: PMC9176689
- DOI: 10.1177/03635465221074662
Meniscal Treatment as a Predictor of Worse Articular Cartilage Damage on MRI at 2 Years After ACL Reconstruction: The MOON Nested Cohort
Abstract
Background: Patients undergoing anterior cruciate ligament reconstruction (ACLR) are at an increased risk for posttraumatic osteoarthritis (PTOA). While we have previously shown that meniscal treatment with ACLR predicts more radiographic PTOA at 2 to 3 years postoperatively, there are a limited number of similar studies that have assessed cartilage directly with magnetic resonance imaging (MRI).
Hypothesis: Meniscal repair or partial meniscectomy at the time of ACLR independently predicts more articular cartilage damage on 2- to 3-year postoperative MRI compared with a healthy meniscus or a stable untreated tear.
Study design: Cohort study; Level of evidence, 2.
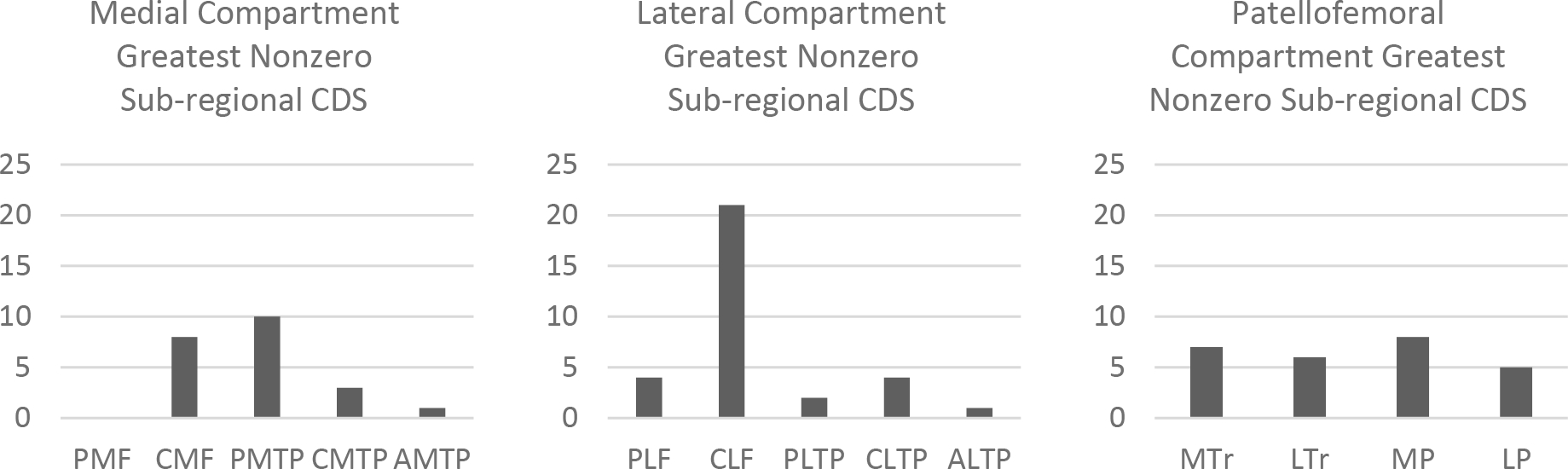
Methods: A consecutive series of patients undergoing ACLR from 1 site within the prospective, nested Multicenter Orthopaedic Outcomes Network (MOON) cohort underwent bilateral knee MRI at 2 to 3 years postoperatively. Patients were aged <36 years without previous knee injuries, were injured while playing sports, and had no history of concomitant ligament surgery or contralateral knee surgery. MRI scans were graded by a board-certified musculoskeletal radiologist using the modified MRI Osteoarthritis Knee Score (MOAKS). A proportional odds logistic regression model was built to predict a MOAKS-based cartilage damage score (CDS) relative to the contralateral control knee for each compartment as well as for the whole knee, pooled by meniscal treatment, while controlling for sex, age, body mass index, baseline Marx activity score, and baseline operative cartilage grade. For analysis, meniscal injuries surgically treated with partial meniscectomy or meniscal repair were grouped together.
Results: The cohort included 60 patients (32 female; median age, 18.7 years). Concomitant meniscal treatment at the time of index ACLR was performed in 17 medial menisci (13 meniscal repair and 4 partial meniscectomy) and 27 lateral menisci (3 meniscal repair and 24 partial meniscectomy). Articular cartilage damage was worse in the ipsilateral reconstructed knee (P < .001). A meniscal injury requiring surgical treatment with ACLR predicted a worse CDS for medial meniscal treatment (medial compartment CDS: P = .005; whole joint CDS: P < .001) and lateral meniscal treatment (lateral compartment CDS: P = .038; whole joint CDS: P = .863). Other predictors of a worse relative CDS included age for the medial compartment (P < .001), surgically observed articular cartilage damage for the patellofemoral compartment (P = .048), and body mass index (P = .007) and age (P = .020) for the whole joint.
Conclusion: A meniscal injury requiring surgical treatment with partial meniscectomy or meniscal repair at the time of ACLR predicted worse articular cartilage damage on MRI at 2 to 3 years after surgery. Further research is required to differentiate between the effects of partial meniscectomy and meniscal repair.
Keywords: MRI; anterior cruciate ligament reconstruction; meniscus; posttraumatic osteoarthritis.
Figures







Similar articles
-
Articular Cartilage and Meniscus Predictors of Patient-Reported Outcomes 10 Years After Anterior Cruciate Ligament Reconstruction: A Multicenter Cohort Study.Am J Sports Med. 2021 Sep;49(11):2878-2888. doi: 10.1177/03635465211028247. Epub 2021 Jul 29. Am J Sports Med. 2021. PMID: 34324369 Free PMC article.
-
Predictors of Radiographic Osteoarthritis 2 to 3 Years After Anterior Cruciate Ligament Reconstruction: Data From the MOON On-site Nested Cohort.Orthop J Sports Med. 2019 Aug 30;7(8):2325967119867085. doi: 10.1177/2325967119867085. eCollection 2019 Aug. Orthop J Sports Med. 2019. PMID: 31516911 Free PMC article.
-
Differences in the Lateral Compartment Joint Space Width After Anterior Cruciate Ligament Reconstruction: Data From the MOON Onsite Cohort.Am J Sports Med. 2018 Mar;46(4):876-882. doi: 10.1177/0363546517751139. Epub 2018 Feb 2. Am J Sports Med. 2018. PMID: 29394877 Free PMC article.
-
Single-stage repair of displaced bucket-handle meniscal tears with anterior cruciate ligament reconstruction leads to good meniscal survivorship : a retrospective cohort study.Bone Joint J. 2022 Jun;104-B(6):680-686. doi: 10.1302/0301-620X.104B6.BJJ-2021-1340.R2. Bone Joint J. 2022. PMID: 35638209 Review.
-
Earlier anterior cruciate ligament reconstruction is associated with a decreased risk of medial meniscal and articular cartilage damage in children and adolescents: a systematic review and meta-analysis.Knee Surg Sports Traumatol Arthrosc. 2018 Dec;26(12):3738-3753. doi: 10.1007/s00167-018-5012-5. Epub 2018 Jun 6. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 29876862
Cited by
-
The PIKASO trial (Preventing Injured Knees from Osteoarthritis: Severity Outcomes): Rationale and design features for a randomized controlled trial.Osteoarthr Cartil Open. 2024 Dec 23;7(1):100563. doi: 10.1016/j.ocarto.2024.100563. eCollection 2025 Mar. Osteoarthr Cartil Open. 2024. PMID: 39867299 Free PMC article.
-
Teaming up to overcome challenges toward translation of new therapeutics for osteoarthritis.J Orthop Res. 2024 Dec;42(12):2659-2672. doi: 10.1002/jor.25944. Epub 2024 Aug 5. J Orthop Res. 2024. PMID: 39103981
-
Chondral Injury Associated With ACL Injury: Assessing Progressive Chondral Degeneration With Morphologic and Quantitative MRI Techniques.Sports Health. 2024 Sep-Oct;16(5):722-734. doi: 10.1177/19417381231205276. Epub 2023 Oct 25. Sports Health. 2024. PMID: 37876228 Free PMC article.
-
Management of Meniscus Pathology with Concomitant Anterior Cruciate Ligament Injury.Curr Rev Musculoskelet Med. 2024 Aug;17(8):321-334. doi: 10.1007/s12178-024-09906-x. Epub 2024 Jun 1. Curr Rev Musculoskelet Med. 2024. PMID: 38822979 Free PMC article. Review.
-
Effect of Concomitant Lateral Meniscal Management on ACL Reconstruction Revision Rate and Secondary Meniscal and Cartilaginous Injuries.Am J Sports Med. 2023 Oct;51(12):3142-3148. doi: 10.1177/03635465231194624. Epub 2023 Sep 8. Am J Sports Med. 2023. PMID: 37681530 Free PMC article.
References
-
- Claes S, Hermie L, Verdonk R, Bellemans J, Verdonk P. Is osteoarthritis an inevitable consequence of anterior cruciate ligament reconstruction? A meta-analysis. Knee Surgery, Sport Traumatol Arthrosc 2013;21(9):1967–1976 - PubMed
-
- Culvenor AG, Collins NJ, Guermazi A, et al. Early knee osteoarthritis is evident one year following anterior cruciate ligament reconstruction: A magnetic resonance imaging evaluation. Arthritis Rheumatol 2015;67(4):946–955 - PubMed
-
- Feeley BT, Lau BC. Biomechanics and clinical outcomes of partial meniscectomy. J Am Acad Orthop Surg 2018;26(24):853–863 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
