

Intensive care unit to unit capacity transfers are associated with increased mortality: an observational cohort study on patient transfers in the Swedish Intensive Care Register
- PMID: 35377019
- PMCID: PMC8980179
- DOI: 10.1186/s13613-022-01003-x
Intensive care unit to unit capacity transfers are associated with increased mortality: an observational cohort study on patient transfers in the Swedish Intensive Care Register
Abstract
Background: Transfers from one intensive care unit (ICU) to another ICU are associated with increased length of intensive care and hospital stay. Inter-hospital ICU transfers are carried out for three main reasons: clinical transfers, capacity transfers and repatriations. The aim of the study was to show that different ICU transfers differ in risk-adjusted mortality rate with repatriations having the least risk.
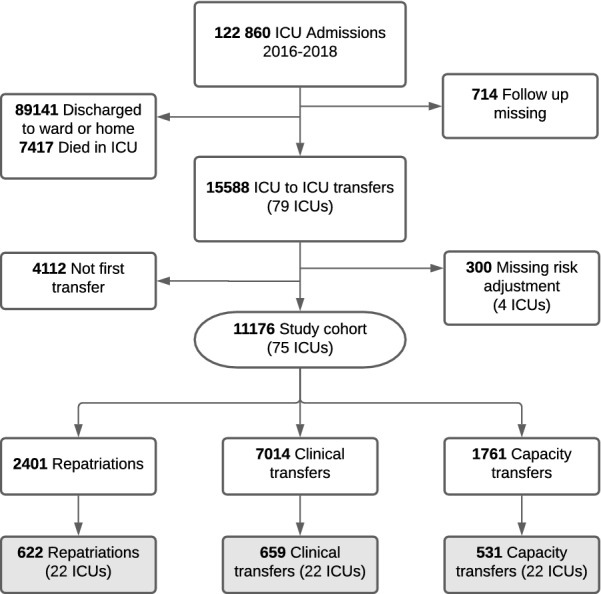
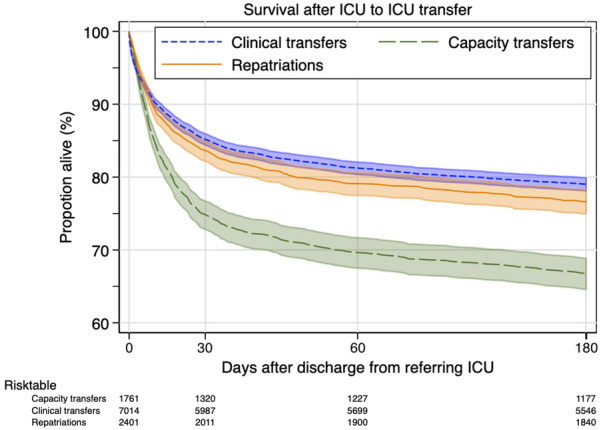
Results: Observational cohort study of adult patients transferred between Swedish ICUs during 3 years (2016-2018) with follow-up ending September 2019. Primary and secondary end-points were survival to 30 days and 180 days after discharge from the first ICU. Data from 75 ICUs in the Swedish Intensive Care Register, a nationwide intensive care register, were used for analysis (89% of all Swedish ICUs), covering local community hospitals, district general hospitals and tertiary care hospitals. We included adult patients (16 years or older) admitted to ICU and subsequently discharged by transfer to another ICU. Only the first admission was used. Exposure was discharge to any other ICU (ICU-to-ICU transfer), whether in the same or in another hospital. Transfers were grouped into three predefined categories: clinical transfer, capacity transfer, and repatriation. We identified 15,588 transfers among 112,860 admissions (14.8%) and analysed 11,176 after excluding 4112 repeat transfer of the same individual and 300 with missing risk adjustment. The majority were clinical transfers (62.7%), followed by repatriations (21.5%) and capacity transfers (15.8%). Unadjusted 30-day mortality was 25.0% among capacity transfers compared to 14.5% and 16.2% for clinical transfers and repatriations, respectively. Adjusted odds ratio (OR) for 30-day mortality were 1.25 (95% CI 1.06-1.49 p = 0.01) for capacity transfers and 1.17 (95% CI 1.02-1.36 p = 0.03) for clinical transfers using repatriation as reference. The differences remained 180 days post-discharge.
Conclusions: There was a large proportion of ICU-to-ICU transfers and an increased odds of dying for those transferred due to other reasons than repatriation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
