

Cost-effectiveness of Robotic-Assisted Radical Prostatectomy for Localized Prostate Cancer in the UK
- PMID: 35377424
- PMCID: PMC8980901
- DOI: 10.1001/jamanetworkopen.2022.5740
Cost-effectiveness of Robotic-Assisted Radical Prostatectomy for Localized Prostate Cancer in the UK
Abstract
Importance: The cost-effectiveness of different surgical techniques for radical prostatectomy remains a subject of debate. Emergence of recent critical clinical data and changes in surgical equipment costs due to their shared use by different clinical specialties necessitate an updated cost-effectiveness analysis in a centralized, largely government-funded health care system such as the UK National Health Service (NHS).
Objective: To compare robotic-assisted radical prostatectomy (RARP) with open radical prostatectomy (ORP) and laparoscopic-assisted radical prostatectomy (LRP) using contemporary data on clinical outcomes, costs, and surgical volumes in the UK.
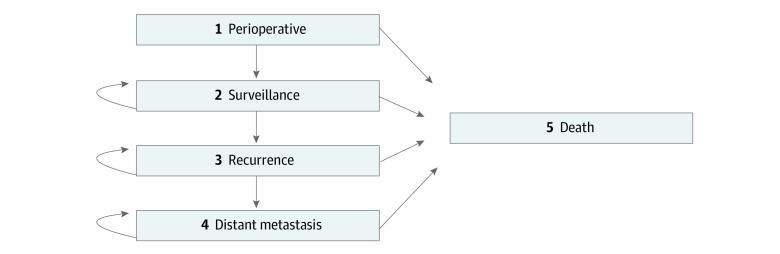
Design, setting, and participants: This economic analysis used a Markov model developed to compare the cost-effectiveness of RARP, LRP, and ORP to treat localized prostate cancer. The model was constructed from the perspective of the UK NHS. The model simulated 65-year-old men who underwent radical prostatectomy for localized prostate cancer and were followed up for a 10-year period. Data were analyzed from May 1, 2020, to July 31, 2021.
Exposures: Robotic-assisted radical prostatectomy, LRP, and ORP.
Main outcomes and measures: Quality-adjusted life-years (QALYs), costs (direct medical costs and costs outside the NHS), and incremental cost-effectiveness ratios (ICERs).
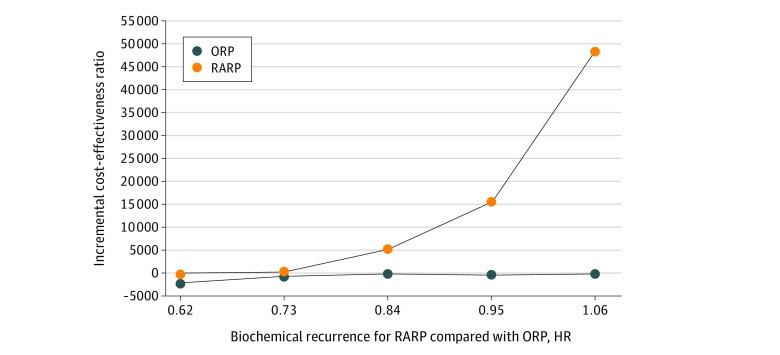
Results: Compared with LRP, RARP cost £1785 (US $2350) less and had 0.24 more QALYs gained; thus, RARP was a dominant option compared with LRP. Compared with ORP, RARP had 0.12 more QALYs gained but cost £526 (US $693) more during the 10-year time frame, resulting in an ICER of £4293 (US $5653)/QALY. Because the ICER was below the £30 000 (US $39 503) willingness-to-pay threshold, RARP was more cost-effective than ORP in the UK. The most sensitive variable influencing the cost-effectiveness of RARP was the lower risk of biochemical recurrence (BCR). Scenario analysis indicated RARP would remain more cost-effective than ORP as long as the BCR hazard ratios comparing RARP vs ORP were less than 0.99.
Conclusions and relevance: These findings suggest that in the UK, RARP has an ICER lower than the willingness-to-pay threshold and thus is likely a cost-effective surgical treatment option for patients with localized prostate cancer compared with ORP and LRP. The results were mainly driven by the lower risk of BCR for RARP. These findings may differ in other health care settings where different thresholds and costs may apply.
Conflict of interest statement
Figures
Comment in
-
Cost-effectiveness of Robotic-Assisted Prostatectomy in the UK-Are We Doing Enough?JAMA Netw Open. 2022 Apr 1;5(4):e225747. doi: 10.1001/jamanetworkopen.2022.5747. JAMA Netw Open. 2022. PMID: 35377430 No abstract available.
References
-
- Cancer Research UK . Prostate cancer statistics. 2021. Accessed July 29, 2021. https://www.cancerresearchuk.org/health-professional/cancer-statistics/s...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
