

Up to 8-year follow-up from RESONATE-2: first-line ibrutinib treatment for patients with chronic lymphocytic leukemia
- PMID: 35377947
- PMCID: PMC9198904
- DOI: 10.1182/bloodadvances.2021006434
Up to 8-year follow-up from RESONATE-2: first-line ibrutinib treatment for patients with chronic lymphocytic leukemia
Abstract
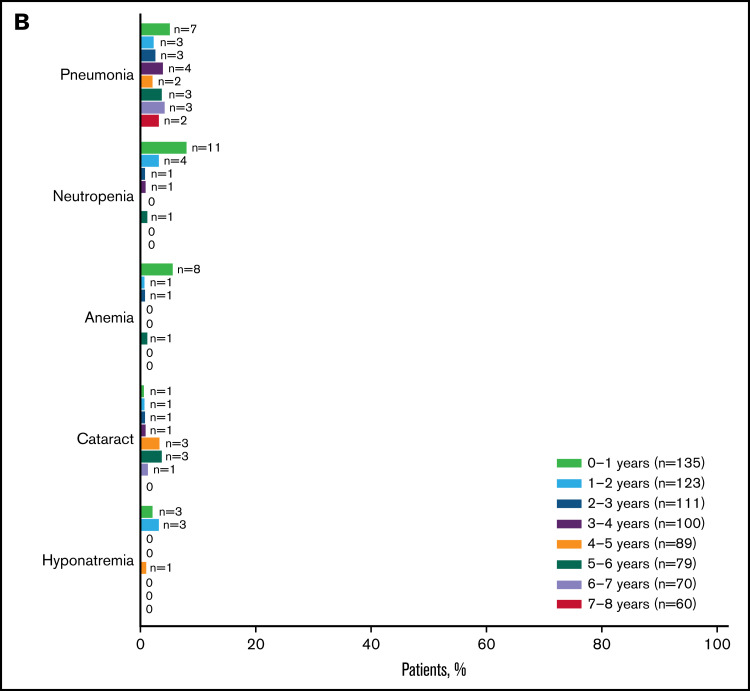
We report long-term follow-up from the RESONATE-2 phase 3 study of the once-daily Bruton's tyrosine kinase inhibitor ibrutinib, which is the only targeted therapy with significant progression-free survival (PFS) and overall survival (OS) benefit in multiple randomized chronic lymphocytic leukemia (CLL) studies. Patients (≥65 years) with previously untreated CLL, without del(17p), were randomly assigned 1:1 to once-daily ibrutinib 420 mg until disease progression/unacceptable toxicity (n = 136) or chlorambucil 0.5-0.8 mg/kg ≤12 cycles (n = 133). With up to 8 years of follow-up (range, 0.1-96.6 months; median, 82.7 months), significant PFS benefit was sustained for ibrutinib vs chlorambucil (hazard ratio [HR], 0.154; 95% confidence interval [CI], 0.108-0.220). At 7 years, PFS was 59% for ibrutinib vs 9% for chlorambucil. PFS benefit was also observed for ibrutinib- vs chlorambucil-randomized patients with high-risk genomic features: del(11q) (HR, 0.033; 95% CI, 0.010-0.107) or unmutated immunoglobulin heavy chain variable region (HR, 0.112; 95% CI, 0.065-0.192). OS at 7 years was 78% with ibrutinib. Prevalence of adverse events (AEs) was consistent with previous 5-year follow-up. Ibrutinib dosing was held (≥7 days) for 79 patients and reduced for 31 patients because of AEs; these AEs resolved or improved in 85% (67 of 79) and 90% (28 of 31) of patients, respectively. With up to 8 years of follow-up, 42% of patients remain on ibrutinib. Long-term RESONATE-2 data demonstrate sustained benefit with first-line ibrutinib treatment for CLL, including for patients with high-risk genomic features. These trials were registered at www.clinicaltrials.gov as #NCT01722487 and #NCT01724346.
© 2022 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Figures







References
-
- Galton DA, Wiltshaw E, Szur L, Dacie JV. The use of chlorambucil and steroids in the treatment of chronic lymphocytic leukaemia. Br J Haematol. 1961;7(1):73-98. - PubMed
-
- Pharmacyclics LLC, an AbbVie Company. Imbruvica (ibrutinib) prescribing information. Sunnyvale, CA: Pharmacyclics LLC, an AbbVie Company; 2020.
-
- Kipps TJ, Fraser G, Coutre SE, et al. Long-term studies assessing outcomes of ibrutinib therapy in patients with del(11q) chronic lymphocytic leukemia. Clin Lymphoma Myeloma Leuk. 2019;19(11):715-722. - PubMed
