

Intramedullary Spinal Cord Lesions: A Single-Center Experience
- PMID: 35378585
- PMCID: PMC8987546
- DOI: 10.14245/ns.2143190.595
Intramedullary Spinal Cord Lesions: A Single-Center Experience
Abstract
Objective: Spinal cord tumors constitute a small part of spinal surgery owing to their rarity. This retrospective study describes their current management.
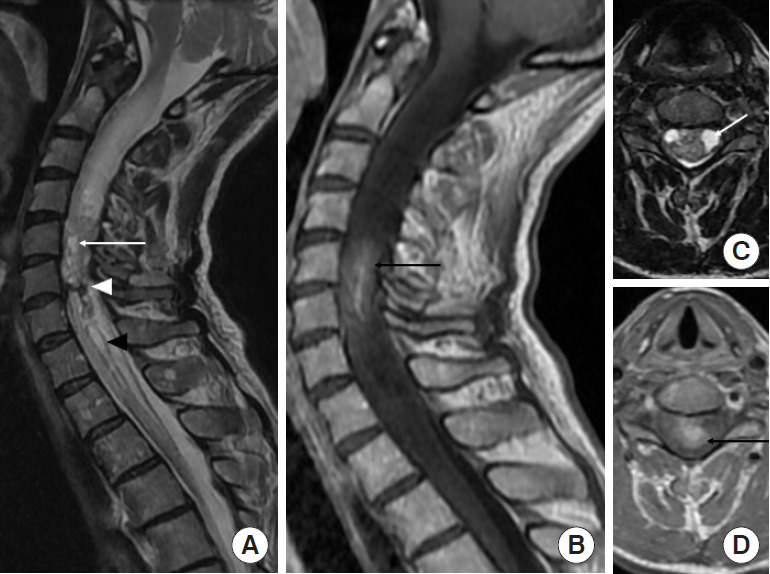
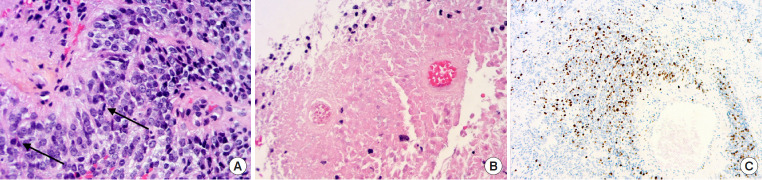
Methods: Forty-eight patients were treated for an intramedullary tumor between 2014 and 2020 at a single institution. Patients' files were retrospectively studied. We detailed clinical status according to neurological deficit and ambulatory ability using the modified McCormick Scale, radiological features like number of levels, associated syringomyelia, surgical technique with or without intraoperative electrophysiological monitoring, pathological findings, and postoperative outcome.
Results: The median age of this population was 43 years, including 5 patients under 18 years. The median delay before first neurosurgical contact was 3 months after the first clinical complaint. Treatment was gross total resection in 43.8%, subtotal resection in 50.0%, and biopsy in 6.2%. A laminectomy was performed for all the patients except 2 operated using the laminoplasty technique. Pathological findings were ependymoma in 43.8%, hemangioblastoma in 20.8%, and pilocytic astrocytoma in 10.4%. Six patients were reoperated for a tumor recurrence less than 2 years after the first surgical resection. One patient was reoperated for a postoperative cervical kyphosis.
Conclusion: Intramedullary tumors are still a challenging disease and they are treated by various surgical techniques. They must be managed in a specialized center including a trained surgical, radiological, electrophysiological, and pathological team. Arthrodesis must be discussed before performing extensive laminectomy to avoid postoperative kyphosis.
Keywords: Astrocytoma; Ependymoma; Hemangioblastoma; Intramedullary tumors.
Conflict of interest statement
The authors have nothing to disclose.
Figures

References
-
- Schellinger KA, Propp JM, Villano JL, et al. Descriptive epidemiology of primary spinal cord tumors. J Neurooncol. 2008;87:173–9. - PubMed
-
- Hoshimaru M, Koyama T, Hashimoto N, et al. Results of microsurgical treatment for intramedullary spinal cord ependymomas: analysis of 36 cases. Neurosurgery. 1999;44:264–9. - PubMed
-
- Helgager J, Driver J, Hoffman S, et al. Molecular advances in central nervous system mesenchymal tumors. Surg Pathol Clin. 2020;13:291–303. - PubMed
-
- Hamilton KR, Lee SS, Urquhart JC, et al. A systematic review of outcome in intramedullary ependymoma and astrocytoma. J Clin Neurosci. 2019;63:168–75. - PubMed
LinkOut - more resources
Full Text Sources
