

Comparison of the surgical resection and infarct 5/6 nephrectomy rat models of chronic kidney disease
- PMID: 35379002
- PMCID: PMC9076416
- DOI: 10.1152/ajprenal.00398.2021
Comparison of the surgical resection and infarct 5/6 nephrectomy rat models of chronic kidney disease
Abstract
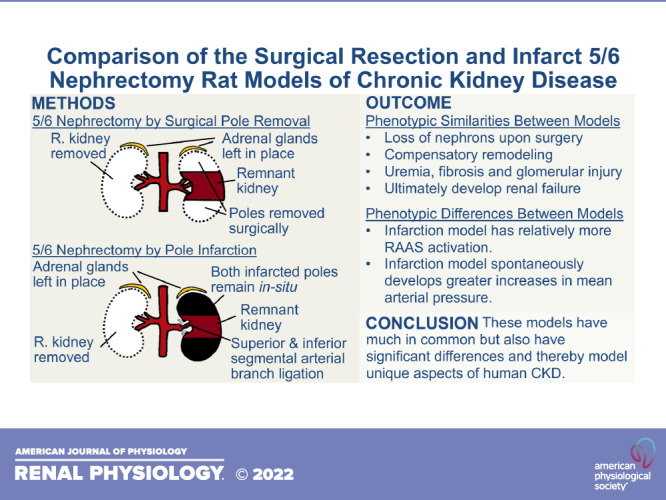
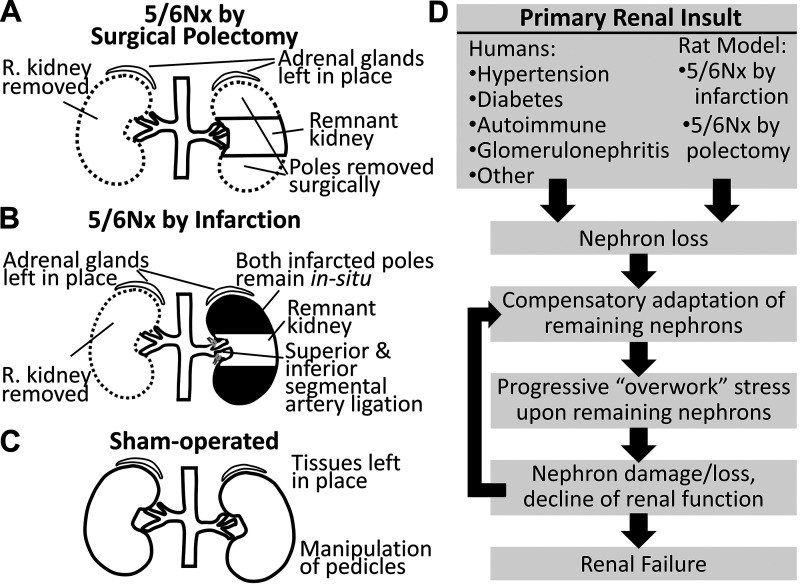
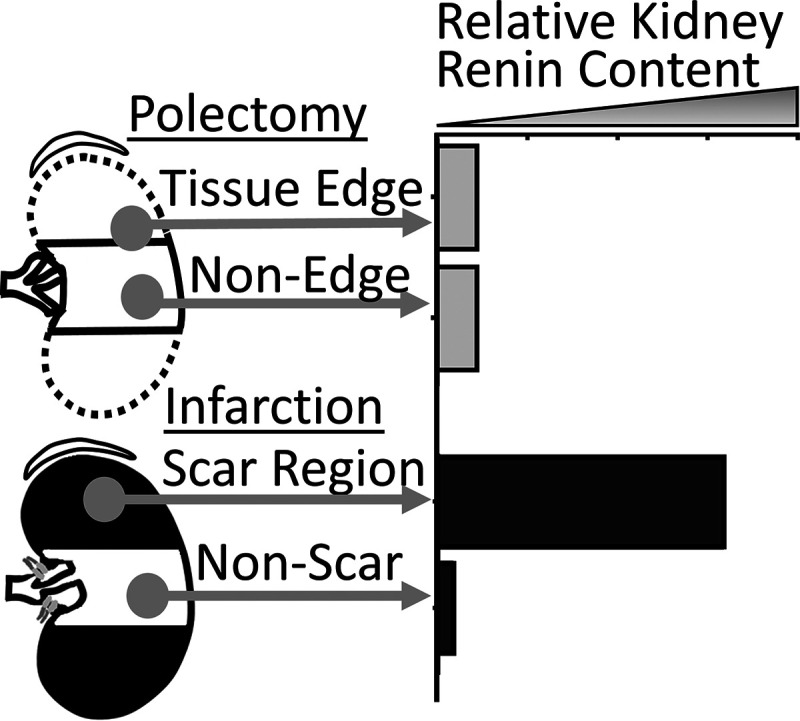
The 5/6 nephrectomy rat remnant kidney model is commonly used to study chronic kidney disease (CKD). This model requires the removal of one whole kidney and two-thirds of the other kidney. The two most common ways of producing the remnant kidney are surgical resection of poles, known as the polectomy model, or ligation of superior and inferior segmental renal arteries, resulting in pole infarction. These models have much in common, but also major phenotypic differences, and thus respectively model unique aspects of human CKD. The purpose of this review is to summarize phenotypic similarities and differences between these two models and their relation to human CKD while emphasizing their vascular phenotype. In this article, we review studies that have evaluated arterial blood pressure, the renin-angiotensin-aldosterone-system, autoregulation, nitric oxide, single-nephron physiology, angiogenic and antiangiogenic factors, and capillary rarefaction in these two models. In terms of phenotypic similarities, both models spontaneously develop hallmarks of human CKD including uremia, fibrosis, capillary rarefaction, and progressive renal function decline. They both undergo whole organ hypertrophy, hyperfiltration of functional nephrons, reduced renal expression of vascular endothelial growth factor, increased renal expression of antiangiogenic thrombospondin-1, impaired renal autoregulation, and abnormal vascular nitric oxide physiology. In terms of key phenotypic differences, the infarction model develops rapid-onset, moderate to severe systemic hypertension and the polectomy model develops early normotension followed by mild to moderate hypertension. Rats subjected to the infarction model have a markedly more active renin-angiotensin-aldosterone system. Comparison of these two models facilitates understanding of how they can be used for studying CKD pathophysiology.
Keywords: 5/6 nephrectomy; autoregulation; blood pressure; chronic kidney disease; renin-angiotensin-aldosterone system.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Chuppa S, Liang M, Liu P, Liu Y, Casati MC, Cowley AW, Patullo L, Kriegel AJ. MicroRNA-21 regulates peroxisome proliferator-activated receptor α, a molecular mechanism of cardiac pathology in cardiorenal syndrome type 4. Kidney Int 93: 375–389, 2018. doi: 10.1016/j.kint.2017.05.014. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical