

MTAP deficiency creates an exploitable target for antifolate therapy in 9p21-loss cancers
- PMID: 35379845
- PMCID: PMC8980015
- DOI: 10.1038/s41467-022-29397-z
MTAP deficiency creates an exploitable target for antifolate therapy in 9p21-loss cancers
Abstract
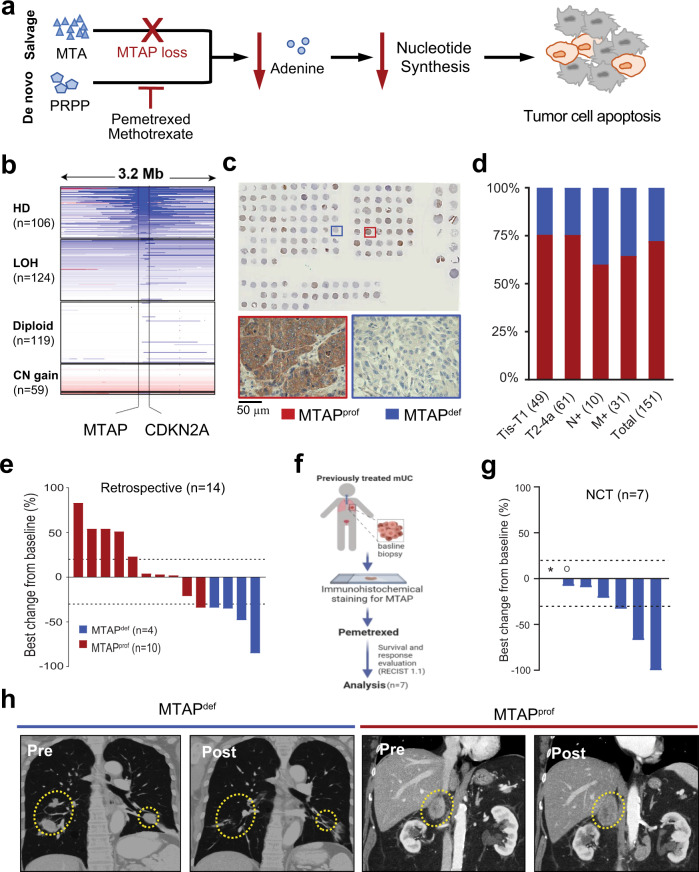
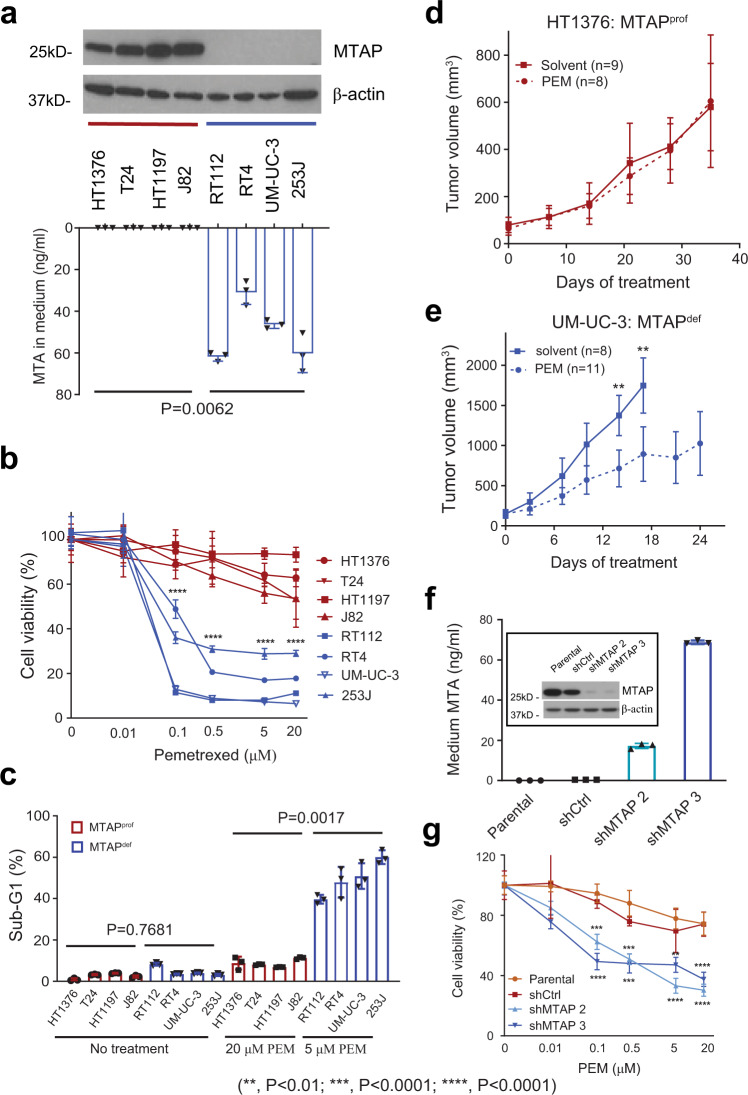
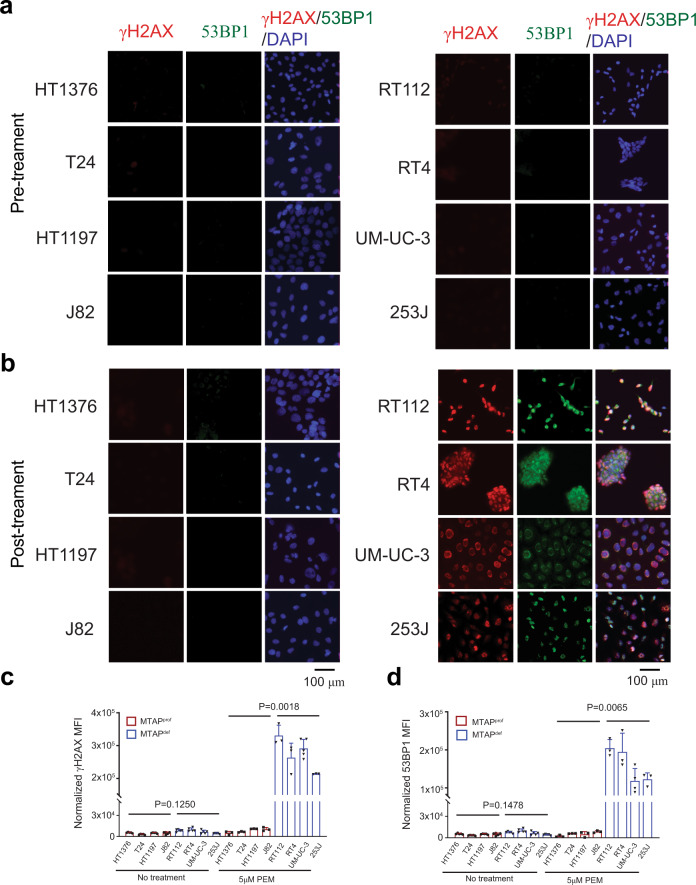
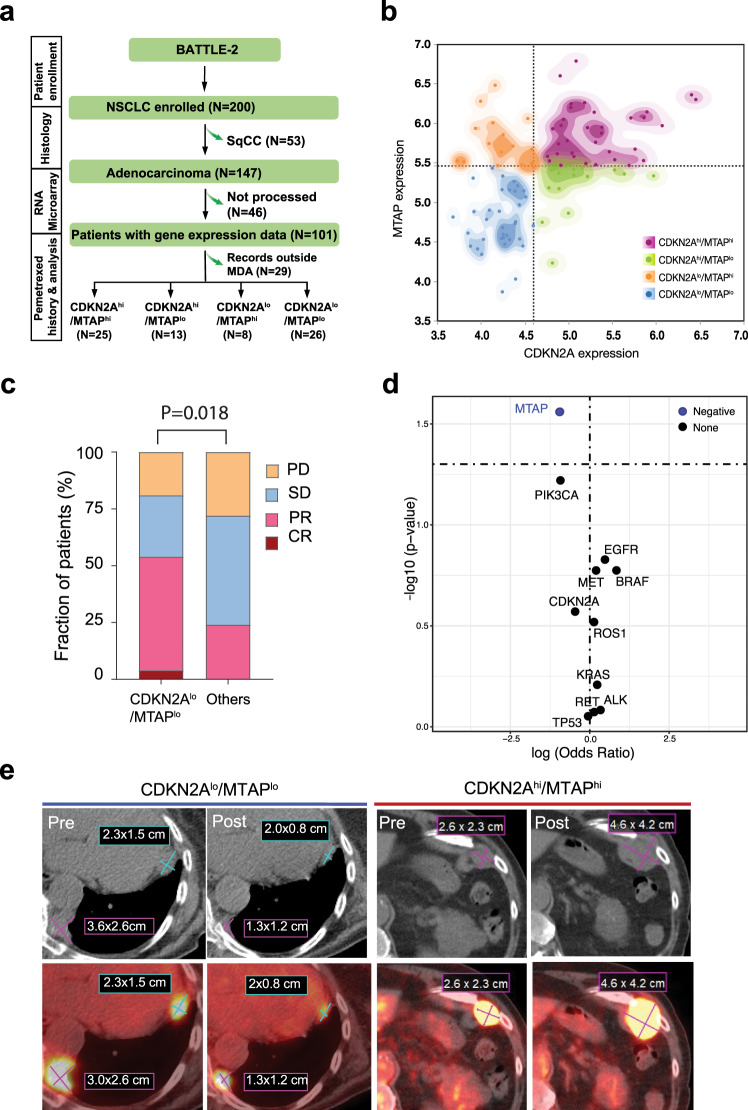
Methylthioadenosine phosphorylase, an essential enzyme for the adenine salvage pathway, is often deficient (MTAPdef) in tumors with 9p21 loss and hypothetically renders tumors susceptible to synthetic lethality by antifolates targeting de novo purine synthesis. Here we report our single arm phase II trial (NCT02693717) that assesses pemetrexed in MTAPdef urothelial carcinoma (UC) with the primary endpoint of overall response rate (ORR). Three of 7 enrolled MTAPdef patients show response to pemetrexed (ORR 43%). Furthermore, a historic cohort shows 4 of 4 MTAPdef patients respond to pemetrexed as compared to 1 of 10 MTAP-proficient patients. In vitro and in vivo preclinical data using UC cell lines demonstrate increased sensitivity to pemetrexed by inducing DNA damage, and distorting nucleotide pools. In addition, MTAP-knockdown increases sensitivity to pemetrexed. Furthermore, in a lung adenocarcinoma retrospective cohort (N = 72) from the published BATTLE2 clinical trial (NCT01248247), MTAPdef associates with an improved response rate to pemetrexed. Our data demonstrate a synthetic lethal interaction between MTAPdef and de novo purine inhibition, which represents a promising therapeutic strategy for larger prospective trials.
© 2022. The Author(s).
Conflict of interest statement
Dr. Shah has honorarium with Pfizer, BMS, Exelixis and research funding from BMS, Eisai, and EMD Serono. Dr. Siefker-Radtke serves as a consultant for Janssen, Merck, the National Comprehensive Cancer Network, Lilly, Bristol-Myers Squibb, AstraZeneca, BioClin Therapeutics, Bavarian Nordic, Seattle Genetics, Nektar, Genentech, Inovio Pharmaceuticals, and EMD Serono. Dr. Siefker-Radtke has received research funding from the National Institute of Health, Michael and Sherry Sutton Fund for Urothelial Cancer, Janssen, Takeda, Bristol-Myers Squibb, BioClin Therapeutics, and Nektar. Dr. Campbell has served as a consultant or has provided non-branded educational lectures with honorarium with Pfizer, EMD Serono, AstraZeneca, Eisai, Apricity, Roche, Bristol Myers Squibb, and Merck. Dr. Gao serves as a consultant for ARMO Biosciences, AstraZeneca, Jounce, Nektar, and Pfizer. Dr. Msaouel has received honoraria for service on a Scientific Advisory Board for Mirati Therapeutics, Exelixis, and BMS, consulting for Axiom Healthcare Strategies, non-branded educational programs supported by Exelixis and Pfizer, and research funding for clinical trials from Takeda, BMS, Mirati Therapeutics, Gateway for Cancer Research, and UT MD Anderson Cancer Center. Jack A. Roth has consultancy, stock, Genprex, Inc.; patents issued and pending. Dr. Ho has received honoraria from Exelixis, Genentech, EMD-Serono, Pfizer, Macrogenics, Cardinal Health, Ipsen, and Aveo. The remaining authors declare no conflicts of interest.
Figures
References
-
- Powles T, et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature. 2014;515:558. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
