

Validation and quantification of left ventricular function during exercise and free breathing from real-time cardiac magnetic resonance images
- PMID: 35379859
- PMCID: PMC8979972
- DOI: 10.1038/s41598-022-09366-8
Validation and quantification of left ventricular function during exercise and free breathing from real-time cardiac magnetic resonance images
Abstract
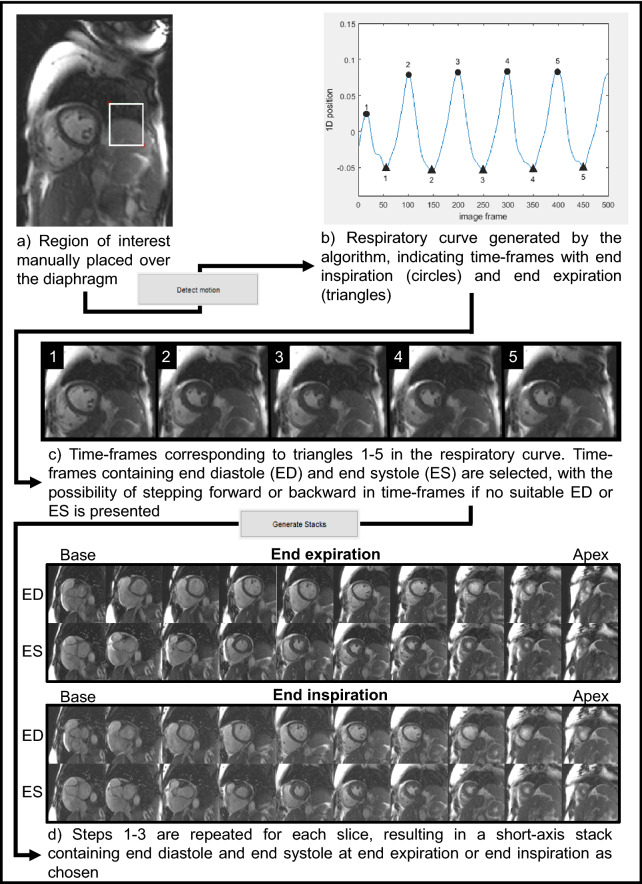
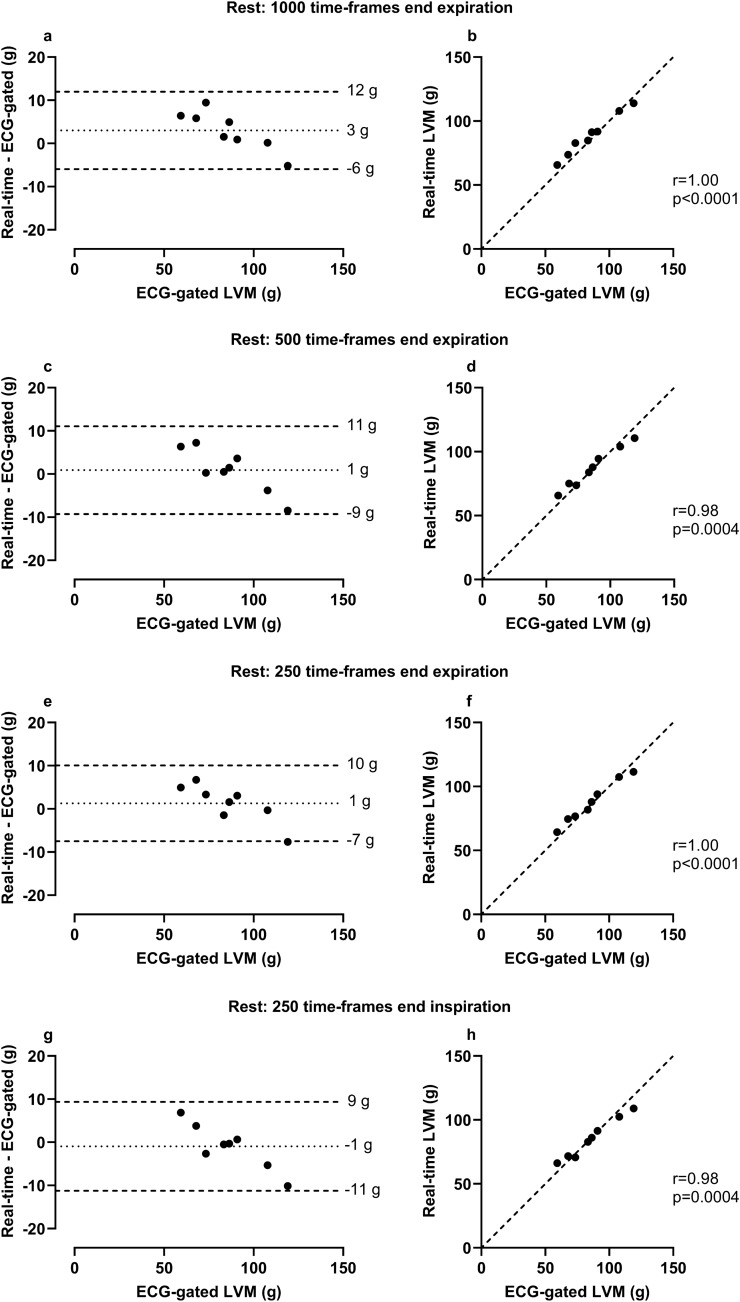
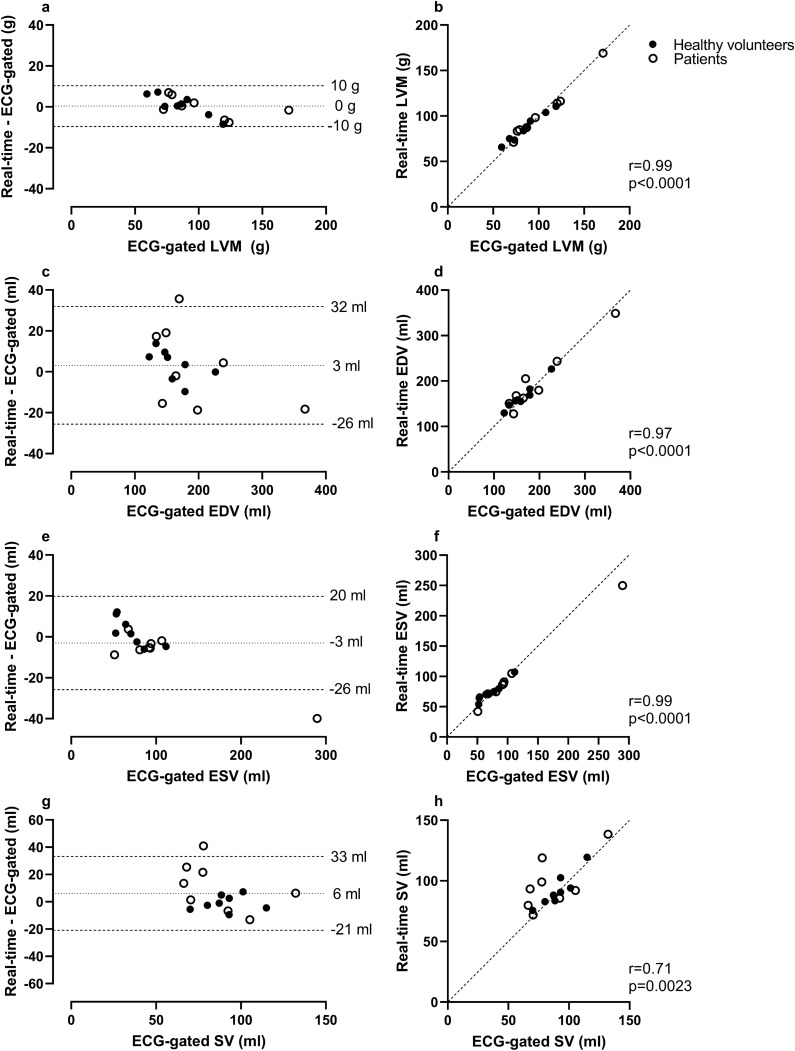
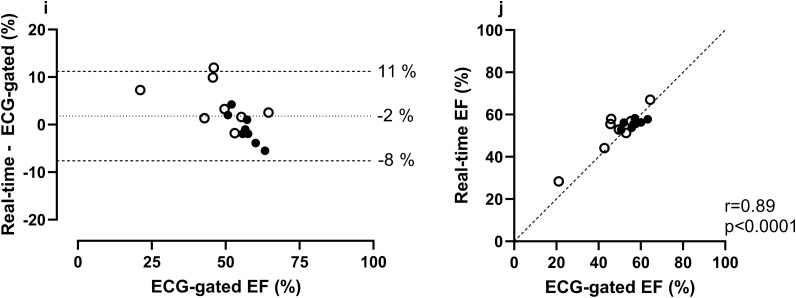
Exercise cardiovascular magnetic resonance (CMR) can unmask cardiac pathology not evident at rest. Real-time CMR in free breathing can be used, but respiratory motion may compromise quantification of left ventricular (LV) function. We aimed to develop and validate a post-processing algorithm that semi-automatically sorts real-time CMR images according to breathing to facilitate quantification of LV function in free breathing exercise. A semi-automatic algorithm utilizing manifold learning (Laplacian Eigenmaps) was developed for respiratory sorting. Feasibility was tested in eight healthy volunteers and eight patients who underwent ECG-gated and real-time CMR at rest. Additionally, volunteers performed exercise CMR at 60% of maximum heart rate. The algorithm was validated for exercise by comparing LV mass during exercise to rest. Respiratory sorting to end expiration and end inspiration (processing time 20 to 40 min) succeeded in all research participants. Bias ± SD for LV mass was 0 ± 5 g when comparing real-time CMR at rest, and 0 ± 7 g when comparing real-time CMR during exercise to ECG-gated at rest. This study presents a semi-automatic algorithm to retrospectively perform respiratory sorting in free breathing real-time CMR. This can facilitate implementation of exercise CMR with non-ECG-gated free breathing real-time imaging, without any additional physiological input.
© 2022. The Author(s).
Conflict of interest statement
EH is the founder of Medviso AB, Lund, Sweden, which sells a commercial version of Segment. The other authors declare that they have no competing interests.
Figures


References
-
- Boesiger P, Maier SE, Kecheng L, Scheidegger MB, Meier D. Visualization and quantification of the human blood flow by magnetic resonance imaging. J. Biomech. 1992;25:55–67. - PubMed
-
- Hundley WG, et al. Quantitation of cardiac output with velocity-encoded, phase-difference magnetic resonance imaging. Am. J. Cardiol. 1995;75:1250–1255. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
