

Conservative initial postoperative anticoagulation strategy after HeartMate 3 left ventricular assist device implantation
- PMID: 35380415
- PMCID: PMC9475015
- DOI: 10.1007/s12471-022-01671-1
Conservative initial postoperative anticoagulation strategy after HeartMate 3 left ventricular assist device implantation
Abstract
Introduction: Although anticoagulation therapy is mandated after implantation of a left ventricular assist device (LVAD), postoperative bleedings and reoperations occur relatively frequently and are associated with worse outcomes. We evaluated the use of a conservative postoperative anticoagulation protocol in patients implanted with a HeartMate 3 (HM3) LVAD.
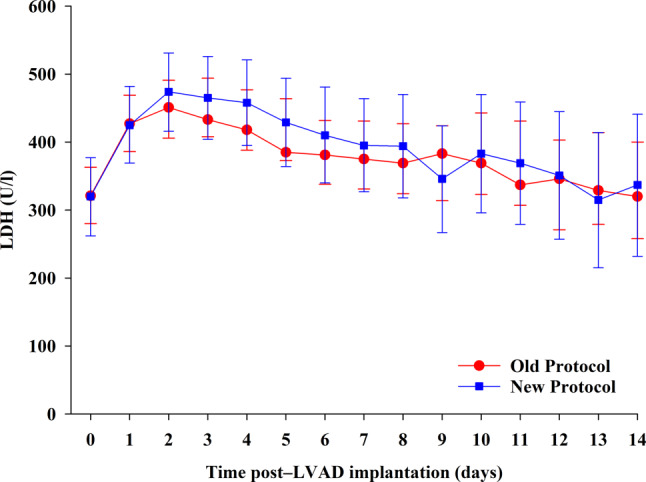
Methods: In a single-centre retrospective analysis of postoperative outcomes after HM3 LVAD implantation, a standard (old) anticoagulation protocol (i.e. early, full-dose anticoagulation with low-molecular weight heparin and overlapping vitamin K antagonist) was compared with a new conservative anticoagulation protocol (i.e. slow initiation of vitamin K antagonists without overlapping heparin). Main outcomes were changes in international normalised ratio (INR), lactate dehydrogenase (LDH), bleeding and/or tamponade events requiring reoperation, length of stay and adverse events.
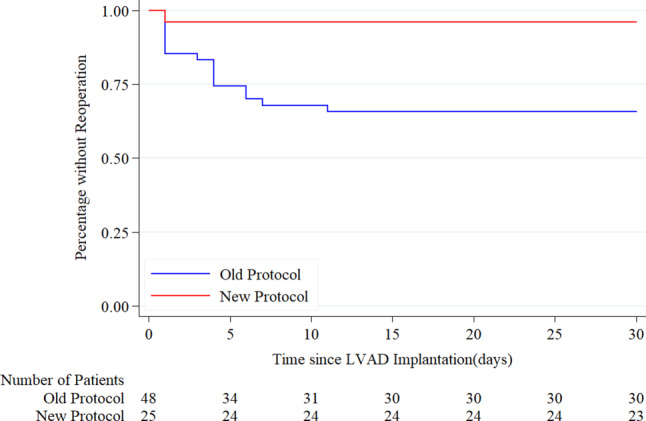
Results: In total, 73 patients (48 in old vs 25 in new protocol group) were evaluated. Mean age was 56 years (standard deviation 13) and most patients (78%) were males. Changes in INR and LDH in the first 14 days were similar in both groups (p = 0.50 and p = 0.997 for interaction, respectively). Number of bleeding/tamponade events requiring reoperation was lower in the new than in the old protocol group (4% vs 33%, p = 0.005). Postoperative 30-day mortality was similar, and we observed no thromboembolic events. Median (25th-75th percentiles) total length of postoperative hospital stay (27 (25-41) vs 21 (19-27) days, p < 0.001) and length of intensive care unit stay (5 (2-9) vs 2 (2-5) days, p = 0.022) were significantly shorter in the new protocol group.
Conclusion: These retrospective data suggest that conservative slow initiation of anticoagulation therapy after HM3 LVAD implantation is associated with less bleeding/tamponade events requiring reoperation, a similar safety profile and a shorter duration of stay than the currently advised standard anticoagulation protocol.
Keywords: Anticoagulation; HeartMate 3; LVAD.
© 2022. The Author(s).
Conflict of interest statement
K. Damman has received speaker fees from Abbott. S.A.J. van den Broek, G. Mecozzi, J.M. Droogh, E. Metz, A. Oude Lansink, J.A. Krikken, M.E. Erasmus and M. Kuijpers declare that they have no competing interests.
Figures

References
-
- Authors/Task Force Members, Document Reviewers 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18:891–975. doi: 10.1002/ejhf.592. - DOI - PubMed
-
- MCS Working Group Dutch Society of Cardiology/Cardiothoracic Surgery (NVVC/NVT).. www.nvvc.nl/Richtlijnen/Consensus-LVAD-2019-Okt-2019-Final.pdf. Accessed july 1st 2021
LinkOut - more resources
Full Text Sources
