

Blunt Cardiac Injury in Patients With Sternal Fractures
- PMID: 35382179
- PMCID: PMC8977059
- DOI: 10.7759/cureus.22841
Blunt Cardiac Injury in Patients With Sternal Fractures
Abstract
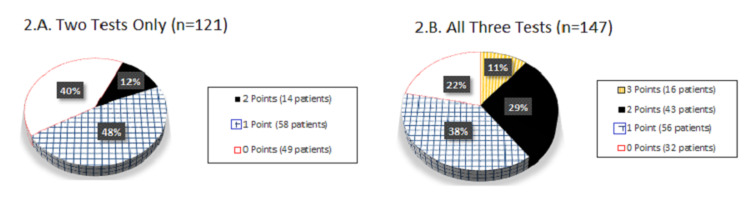
Background Blunt cardiac injury (BCI) is a possible consequence of sternal fractures (SF). There is a scarcity of studies addressing BCI in patients with different types of SF and with pre-existing cardiac conditions. The goal of this study was to delineate diagnostic patterns of BCI in different cohorts of SF patients. Methods This retrospective cohort study included 380 blunt trauma patients admitted to two level 1 trauma centers between January 2015 and March 2020 with radiologically confirmed SF. Electrocardiography, cardiac enzymes and echocardiography were evaluated for BCI diagnosis. Analyzed variables included: age, comorbidities, injury severity score, Glasgow coma score, type of SF (isolated, combined, displaced), incidence of traumatic brain injury, co-injuries, retrosternal hematoma, intensive care unit admissions, hospital lengths of stay, and mortality. Results In 380 SF patients there were 250 (66%) females and 130 (34%) males and the mean age was 63 years old. Electrocardiography was done in all patients, cardiac enzymes in 234 (62%) and echocardiography in 181 (48%). BCI was diagnosed in 19 (5%) of patients, all having combined SF. BCI patients had higher injury severity score (mean 18.4) and 14 (74%) had pulmonary co-injuries. Multivariable analysis confirmed pulmonary co-injuries as a statistically significant predictor of BCI (p<0.001). BCI patients compared to no BCI patients had all three tests (electrocardiography, cardiac enzymes and echocardiography) performed statistically more often (90% vs 36%, p<0.001). SF patients with pre-injury cardiac comorbidities had similar incidence of BCI as without cardiac comorbidities (5% vs 6%, p=0.6). In SF patients with traumatic brain injury, cardiac enzymes (troponin, creatine kinase) were elevated significantly more often compared to patients without traumatic brain injury (58% vs 38%, p=0.02). SF displacement or retrosternal hematoma presence were not associated with BCI. Mortality in SF patients with BCI versus without was not statistically different (16 vs 9%, p=0.4). Conclusions Blunt cardiac injury is rare in patients with SF. Higher degree of BCI suspicion must be applied in combined SF patients, especially those with pulmonary co-injuries. Cardiac comorbidities did not affect the rate of BCI. Echocardiography for BCI diagnosis is essential in SF patients with traumatic brain injury, as cardiac enzymes may be less informative, however is less important in isolated SF patients. Performing all three diagnostic tests in combined SF patients improves the accuracy of BCI diagnosis.
Keywords: blunt cardiac injury; blunt thoracic trauma; cardiac comorbidities; cardiac contusion; echocardiography; sternal fractures; traumatic brain injury; troponin.
Copyright © 2022, Fokin et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Unusual forms of heart disease. Burchell HB. Circulation. 1954;10:574–579. - PubMed
-
- Determining which patients require evaluation for blunt cardiac injury following blunt chest trauma. Nagy KK, Krosner SM, Roberts RR, Joseph KT, Smith RF, Barrett J. World J Surg. 2001;25:108–111. - PubMed
-
- Cardiovascular injuries associated with sternal fractures. Rashid MA, Ortenwall P, Wikström T. Eur J Surg. 2001;167:243–248. - PubMed
-
- Normal electrocardiography and serum troponin I levels preclude the presence of clinically significant blunt cardiac injury. Velmahos GC, Karaiskakis M, Salim A, Toutouzas KG, Murray J, Asensio J, Demetriades D. J Trauma. 2003;54:45–51. - PubMed
-
- Blunt cardiac injury: a single-center 15-year experience. Gao JM, Li H, Wei GB, et al. Am Surg. 2020;86:354–361. - PubMed
LinkOut - more resources
Full Text Sources